This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Madden, Paramedic. It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). An interesting comment provided by Paramedic Madden is that a few team members initially interpreted the T wave presentation as hyperkalemia, as opposed to occlusive hyperacuity. Physiology.
Date: September 8th, 2021 Reference: Desch et al. Date: September 8th, 2021 Reference: Desch et al. The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation. Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients.
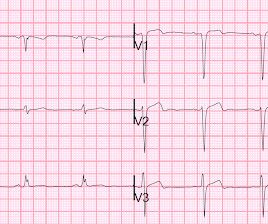
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review provided by Dr. Steve Smith @SmithECGblog I was conducting QA/QI on two very recent cases and was struck by the uniqueness of both. It’s important to stress the presence of a normal QRS (i.e., This ECG immediately struck me as an LAD occlusion.
PARAMEDIC 3 randomized 6,000 (but they were supposed to get to 15,000) patients with out of hospital arrest from multiple EMS agencies in the UK to either an IO or IV to start. A Randomized Trial of Drug Route in Out-of-Hospital Cardiac Arrest. N Engl J Med. 2024 Oct 31:10.1056/NEJMoa2407780. doi: 10.1056/NEJMoa2407780. Epub ahead of print.
Paramedics provided another 3 sprays of nitro, and 6mg of morphine, which reduced but did not resolve the pain. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1] Amsterdam et al.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Expert commentary provided by Dr. Ken Grauer CASE 1 An 82 y/o Male called 911 for sudden onset dizziness while at rest. Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. 2 The astute paramedic recognized this possibility and announced a CODE STEMI. Look at the aortic outflow tract. What do you see? Answer below in the still shot.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al.
Serial ECGs demonstrated dynamic changes diagnostic of ACS (transient STEMI) 4. Even after STEMI (if reperfused, with small amount of myocardium infarcted), and even when the ECG is diagnostic of ACS (as it was the next day), the simultaneous echocardiogram may be normal. Learning Points 1. This was diagnosed as a NonSTEMI. Hypothesis.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review by Dr. Stephen Smith @smithECGblog I was reviewing ECG’s in our LifeNet database and happened upon this one without any knowledge of clinical circumstances. 1] Driver, B. Posterior wall reperfusion T-waves: Wellens’ syndrome of the posterior wall.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review provided by Dr. Steve Smith [link] @SmithECGblog A 72 y/o Male experiences a syncopal episode while seated. This is important because we must rely on the ECG to further elucidate the story when the patient cannot. 3] Meyers, H. 4] Dodd, K. 5] Isnard, R.
Here’s the paramedic ECG (digitized by PMcardio). According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists. paramedic transportation to the ED as “chest pain, STEMI negative” 2.
Medications: FI has a long history of use in the prehospital world, as many agencies were/are reluctant to provide paralytics to paramedics. References: Heffner AC et al. PMID: 23911630 Kim WY et al. PMID: 23911630 Kim WY et al. PMID: 25402500 Forsythe SM et al. PMID: 10631227 Mosier JM et al.
T – He’s got a single grey cannula in situ, and we’ve given him a 5 mg bolus of IiV morphine on the way in The primary survey Thanking the paramedic team, you ask the T&O SHO to proceed with a primary survey. Kulvatunyou N, Bauman ZM, Zein Edine SB, de Moya M, Krause C, Mukherjee K, Gries L, Tang AL, Joseph B, Rhee P.
This was shown to me by a very astute Hennepin paramedic. Although this comes from a Hennepin paramedic, the patient was not brought to Hennepin County Medical Center. It is important for cardiologists to realize that a paramedic may see something they do not. Khan AR, Golwala H, Tripathi A, et al. of this post.
She was found by paramedics with an oxygen saturation of 64%, but could not tolerate BiPAP during transport due to claustrophobia. This presentation clearly indicates more than simple ACS ( A cute C oronary S yndrome ). She awoke in the morning with sharp chest pain which worsened throughout the morning.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content