This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. Studies such as those by Moise et al 14 and Ellis et al 39 have shown that the relative risk of developing an acute myocardial infarction in the territory supplied by an artery with a 70%. He was started on nitro gtt.
Although the attending crews did not consider the ECG pathognomonic for occlusive thrombosis, they nonetheless considered the patient high-risk for ACS and implored him to reconsider. A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. The pathology is now painfully evident.
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. Do NOT give it unless you are committed to the cath lab!! Cath attending is aware. It is a mass delusion.
Based on recent studies, current guidelines recommend that O2 should not be given to non-hypoxemic patients with STEMI or NSTEMI [2,3]. REBEL Cast Ep114 – High Flow O2, Suspected ACS, and Mortality? Click here for Direct Download of the Podcast Paper: Stewart, RAH et al. Low O2 protocol: 3.1% aOR 0.96, 95% CI 0.86
Date: September 8th, 2021 Reference: Desch et al. Date: September 8th, 2021 Reference: Desch et al. Defibrillation is the treatment of choice in these cases but does not often result in sustained ROSC ( Kudenchuk et al 2006). Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients.
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Lindahl et al. From Gue at al. This has resulted in an under-representation of STEMI MINOCA patients in the literature.
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." In fact, Kosuge et al. Stein et al. This is a paper worth reading : Marchik et al. Kosuge et al. Witting et al. of patients with PE and 3.3% of patients without PE.
Many conditions outside of acute coronary syndrome (ACS) mimic ST-elevation myocardial infarction (STEMI), but only a handful of cases have reported ST-elevations (STE) in the setting of pancreatic inflammation where underlying ACS was excluded. 2 Proposed hypothesis as described by Hsu et al., Accessed November 29, 2023.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). There is mixed overlap of ST-segment elevation (STE), ST-segment depression (STD), Hyperacute T waves (HATW), and deWinter pattern (which the ACC regards as a STEMI-equivalent but is better suited under the blanket of OMI).
There were zero patients in this study with a "normal" ECG who had any kind of ACS! So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. Deutch et al.
BP 142/100 HR 90 RR 16 (BBS CTA) SpO2 99 (RA) Dstick 110 My colleagues noted the ST-depression in the respective leads, as well, and STEMI activated to the nearest PCI center. 1] Here is the admitting ED ECG after cancellation of Code STEMI. The EMS crews were correct moving forward with STEMI activation. 1] Driver, B.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. Herzog et al. Khan et al. Take home 1.
The Queen of Hearts agrees: Here the Queen explains why: However, it was not interpreted correctly by the providers: ED interpretation of ECG: "paced rhythm, LBBB but no STEMI pattern." Most large STEMI have peak troponin I in the 20.0 There are hyperacute T-waves in V5 and V6. Next trop in AM. Peak trop 257.97 ng/mL - 80.0
The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Similarly, the OMI paradigm respects ACS as a dynamic process in which ECG changes reflect the phase of myocardial injury and risk stratify which patients may benefit from emergent PCI. Bigger et al. Is there STEMI?
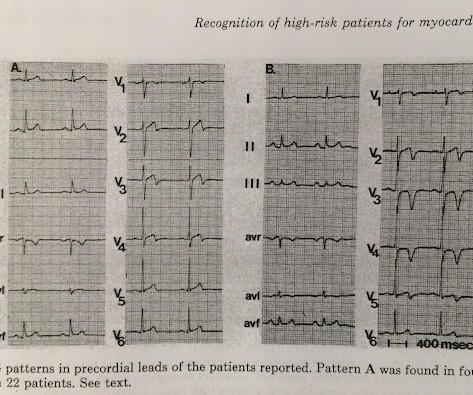
You can see how V1, V2, aVR, and V4R would have ST elevation in either a right ventricular STEMI or with a septal STEMI, and how lateral leads, and even posterior leads, would have reciprocal ST depression. In a 1999 study by Engelen et al. of patients with anterior STEMI, ST elevation of greater than or equal to 3.0
This ECG was read as “No STEMI” with no prior available for comparison. It is true this ECG does not meet STEMI criteria (there is 1.0 Armstrong et al. The Queen of Hearts sees it of course: Still none of these three ECGs meet STEMI criteria. Instead we discussed 5 minute delays for the STEMI(+) OMI patients.
STEMI was activated and the patient went to Cath on arrival. Such aggressive investigation was particularly warranted in this case because of symptoms compatible with ACS, as well as an equally frightening revelation of family history. link] [1] Mirand, D. Canadian Journal of Cardiology, 34 ; 132-145. [2] 2] Aslanger, E.,
Figure 1-1 My colleague, a faithful student of ECG interpretation, handed me the tracing and said that it warranted STEMI activation because of apparent terminal QRS distortion (TQRSD) in V2. Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. His response: “subendocardial ischemia. Anything more on history? POCUS will be helpful.”
Thus, these troponins are very concerning for ACS, and subsequent ones will probably be diagnostic of acute MI. Heitner et al. For this test it is VERY low (very good) at 4% at the 99th percentile -- 26 ng/L, but it will not be so good at a level of 9 ng/L. The troponin is trapped in the myocardium that is not being perfused.
Precordial ST depression may be subendocardial ischemia or posterior STEMI. If you thought it might be a posterior STEMI, then you might have ordered a posterior ECG [change leads V4-V6 around to the back (V7-V9)]. In this case, the patient had failed to take his atenolol in the AM and was having reflex tachycardia in addition to ACS.
But if they do present: The very common presentation of diffuse STD with reciprocal STE in aVR is NOT left main occlusion , though it might be due to sub total LM ACS, but is much more often due to non-ACS conditions, especially demand ischemia. All are, however, clearly massive STEMI. Widimsky P et al.
Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. Lemkes et al. No wall motion abnormality This shows that significant ACS can have ZERO WMA!! Is it normal STE? Eur Heart J 2018.
The precordial ST-depression pattern on this ECG (and in this clinical setting) should immediately raise suspicion of Posterior STEMI! Posterior STEMI occurs in approximately 15-20% of acute MI, but the vast majority of the time it is seen in conjunction with inferior (Infero-Posterior) or lateral (Postero-Lateral) STEMI (1).
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). In our opinion it should not be given in ACS unless you are committed to the cath lab. Am J Emerg Med. 2014;32:e5–e8.
This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. Thelin et al. Mokhtari et al. These include: i ) appreciation of how problematic the definition of “acute STEMI” can be; and , ii ) illustration of how dependence on this definition may result in overlooking acute coronary occlusion.
Troponin T peaked at 2074 ng/L (very high, typical of OMI/STEMI). 3) RV Failure leads to hypotension but NOT pulmonary edema (unlike LV failure) 4) Repeat ECGs, right sided ECG and bedside echo may be helpful in making a diagnosis of ACS. Post PCI the patient became gravely hypotensive and "shocky". The LV EF was 57% at formal echo.
STEMI , ST-segment elevation acute myocardial infarction ). 1 Initial diagnosis of STEMI ECG Management Recommendation Level of evidence A 12-lead ECG should be interpreted immediately (within 10 minutes) at first medical contact. I C If possible, patients should bypass non-PCI centres to a PCI-capable centre.
Because there was proven thrombus (ACS) but the troponin never went above the 99% reference range (and therefore cannot be called MI -- definition of MI requires rise and/or fall of troponin with at least one value above the 99% reference range), this is UNSTABLE ANGINA with ST Elevation.
Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Also note that they allow ST depression c/w posterior MI to be a STEMI equivalent. Kurkciyan et al. Kurkciyan et al.,
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
But beware the few false negatives, especially when there are hyperacute T-waves but no ST elevation (see Case 2 below): Formula to differentiate Normal Variant ST Elevation (Early Repolarization) from Anterior STEMI. 2 or 3 do not rule out unstable angina, even in the era of high sensitivity troponin: this study by Thelin et al.
LVH and the diagnosis of STEMI - how should we apply the current guidelines? In this paper, Dr. Birnbaum writes: "In patients with ACS without LVH, ST depression with negative T waves in the lateral leads is a sign of sub-endocardial ischemia and is an independent predictor of adverse outcome [11 – 13]. Armstrong EJ et al.
Here is an article I wrote: Updates on the ECG in ACS. The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present.
SCAD isn’t rare, especially in women Historically SCAD had been identified in 22% of ACS cases in women. A recent study found that SCAD causes almost 20% of STEMI in young women. Pregnancy is not a common cause of SCAD When ACS occurs in the peripartum period, SCAD is responsible in 43% of cases. A study by Hassan et al.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. Lindahl et al. From Gue at al.
He had no symptoms of ACS. The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS." Physician: "No STEMI."
The provider contacted cardiology to discuss the case, but cardiology "didn't think it was a STEMI, didn't think he needed emergent cath." Canto et al. JAMA 2000) showed that 1/3 of patients with STEMI, and 1/3 of patients with NSTEMI, present without chest pain. The whole paradigm is literally called "STEMI" vs. "NSTEMI."
Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. The ECG only tells you there is ischemia, not the etiology of it. Nevertheless, the clinical situation made other etiologies unlikely. Is this OMI?
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion).
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). LAFB, atrial flutter, anterolateral STEMI(+) OMI. Limkakeng AT.
Had the cardiologists followed NSTEMI or transient STEMI guidelines, which recommend non-urgent cath, the patient could have redeveloped an OMI and had a worse outcome. But this foresight will not be recorded, because the patient was diagnosed as "transient STEMI", even though no ECG ever met STEMI criteria. Take home 1.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content