This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
REBEL Cast Ep114 – High Flow O2, Suspected ACS, and Mortality? PMID: 33653685 Clinical Question: Is there an association between high flow supplementary oxygen and 30-day mortality in patients presenting with a suspected acute coronary syndrome (ACS)? Click here for Direct Download of the Podcast Paper: Stewart, RAH et al.
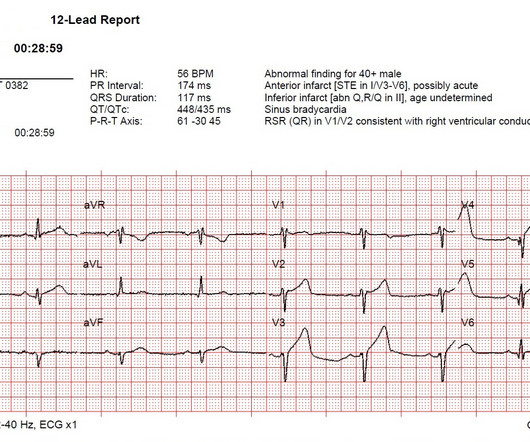
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. looked at consecutive patients with PE, ACS, or neither. What do you think? ng/mL, BNP 2790, and lactate 3.7. Kosuge et al.
His wife contacted the ambulance service after the patient experienced an episode of loss of consciousness. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch).
She was brought in by ambulance and received aspirin and nitroglycerin en route. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. This originally radiated into her left arm. References: 1.
While one may argue that nitro really has no mortality benefit in ACS, I have seen patients with CHF present with hyper tension and inferior S-T elevation, in which the providers were scared to even look at the bottle of nitro. References Kimbrell J, Kreinbrook J, Poke D, Kalosza B, Geldner J, Shekhar AC, Miele A, Bouthillet T, Vega J.
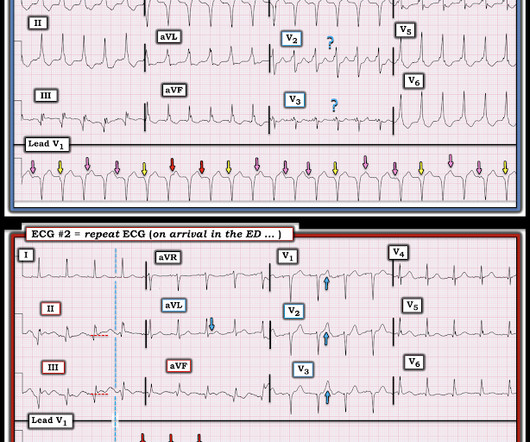
It was during this time that a sudden increase in pulse rate was noted, so another 12 Lead ECG was recorded upon docking the stretcher in the ambulance: There is now 1:1 P:QRS ratio with LBBB. Attending crews then brought the stretcher close and further assisted him to a reclined position of comfort. Hospital transport was unremarkable.
The ambulance report says "BP continued to drop during transport and pt remained cold and clammy." The 3 most common causes of ACS ( A cute C oronary S yndrome ) wit hout evidence of obstructive coronary disease on cath are: i ) Myocarditis ( up to 1/3 of these patients ); ii ) Takotsubo cardiomyopathy; and , iii ) MINOCA.
Assuming the patient has signs and symptoms of ACS, this should be an easy diagnosis. If you’re a paramedic, by obtaining a 12-lead ECG with the first set of vital signs , and not waiting until the patient is in the back of the ambulance, it gives you “another bite at the apple” before you leave the scene.
Grabbing a pristine white table napkin to apply pressure to the wound, Ranulf’s class teacher and expedition leader called the ambulance as chaos descended on the restaurant. Tarquin screamed and pulled the knife straight back out, but blood started to spurt from the decent-sized incision he had accidentally made. The trauma call goes out.
Serial ECGs demonstrated dynamic changes diagnostic of ACS (transient STEMI) 4. Even after STEMI (if reperfused, with small amount of myocardium infarcted), and even when the ECG is diagnostic of ACS (as it was the next day), the simultaneous echocardiogram may be normal. Learning Points 1. This was diagnosed as a NonSTEMI.
On follow-up 1 week later, the patient was doing well, ambulating and playing without significant discomfort. link] Li Z, Krippendorff BF, Sharma S, Walz AC, Lavé T, Shah DK. Following this second dose, the firmness and swelling of the leg improved, and the patient had an otherwise uneventful hospital course. Accessed August 17, 2023.
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. CPR was initiated immediately. It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation.
However, while LSBs have historically been used to attempt spinal immobilization, SMR may be achieved using a scoop stretcher, vacuum splint, ambulance cot, or other similar device to which a patient is safely secured. Both terms refer to the same concept — minimizing unwanted movement of the potentially injured spine.
Assessing the Severity The severity of an electrical burn depends on several factors: the type of current (AC or DC), voltage, the pathway of the current through the body, the duration of contact, and the victim’s overall health. As EMTs, we’re always prepared to address these life-threatening complications alongside the burns.
One must always be careful when looking for "baseline" ECGs, because the prior ECG on file may have been during another ACS event, as this one clearly was. In the ambulance during transport, the patient suddenly suffered VF arrest. Cath lab activation was cancelled but the transfer was accepted for urgent cardiology evaluation.
Patient C, a 27-year-old female with a history of epilepsy, taking valproate and endorsing adherence, is then brought in by ambulance for a witnessed seizure. ACS chemical neuroscience molecule spotlight on Contrave. ACS Chem Neurosci. This is her first seizure in six years. Accessed January 11, 2024. 2011;2(9):484-486.
The nitro she took in the ambulance did not help. Patients like her are the reason we are advocating for a change in the ACS paradigm from STEMI to OMI. While she was in her bed at home, she had sudden onset of left sided chest pain that radiated to her shoulder. The pain was pleuritic, without nausea or diaphoresis.
I B Ambulance personnel must be trained and equipped to identify STEMI and administer fibrinolysis if necessary. I C Glucose-lowering therapy should be considered in ACS patients with glucose levels >10 mmol/L (>180 mg/dL), while episodes of hypoglycaemia (defined as glucose levels <_3.9
After ruling out for ACS, the patient underwent angiography where he was found to have severe stable disease, which was already known. The patient was then sent to the ED for evaluation not by ambulance but driven to the ED by his wife. This would be approximately 95% of the patient's maximum predicted sinus rate.
html ) Despite an undetectable troponin and three normal EKGs, the nature of the patients symptoms and his positive cardiac history warranted concern for ACS. As such, the patient was placed on a heparin drip and transferred by ambulance to a cardiac cath-capable facility.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content