This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
She was brought in by ambulance and received aspirin and nitroglycerin en route. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. This originally radiated into her left arm.
The ambulance report says "BP continued to drop during transport and pt remained cold and clammy." Frick — an all-too-common misconception is that the absence of obstructive coronary disease on cardiac catheterization rules out acute coronary occlusion as the cause of the patient's acute event. This is not the case.
The nitro she took in the ambulance did not help. If she had no risk factors, it is doubtful that she would have developed such extensive coronary artery disease as we see on the angiogram. Patients like her are the reason we are advocating for a change in the ACS paradigm from STEMI to OMI.
His wife contacted the ambulance service after the patient experienced an episode of loss of consciousness. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch).
Background: Historically, we have treated acute coronary syndrome with supplemental oxygen regardless of the patient ’ s oxygen saturation. More recent evidence, however, demonstrates that too much oxygen could be harmful ( AVOID Trial ) by causing coronary vasoconstriction and increasing oxidative stress. Low O2 protocol: 3.1%
Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. Evaluation of T-wave morphology in patients with left bundle branch block and suspected acute coronary syndrome. 3] Meyers, H. 4] Dodd, K.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. looked at consecutive patients with PE, ACS, or neither. What do you think? ng/mL, BNP 2790, and lactate 3.7. Kosuge et al.
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. CPR was initiated immediately. It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation.
Acute coronary occlusion is the most common and most treatable cause of this pattern, but it is not the only cause. Takotsubo, spasm, low flow with a preexisting stable coronary lesion, etc. In the ambulance during transport, the patient suddenly suffered VF arrest.
This page summarises the most current recommendations for the management of acute coronary syndromes with persistent ST-segment elevations (i.e I B Ambulance personnel must be trained and equipped to identify STEMI and administer fibrinolysis if necessary. STEMI , ST-segment elevation acute myocardial infarction ).
After ruling out for ACS, the patient underwent angiography where he was found to have severe stable disease, which was already known. The patient was then sent to the ED for evaluation not by ambulance but driven to the ED by his wife. This would be approximately 95% of the patient's maximum predicted sinus rate.
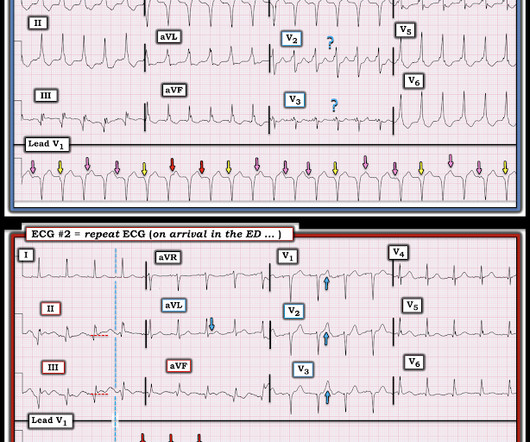
html ) Despite an undetectable troponin and three normal EKGs, the nature of the patients symptoms and his positive cardiac history warranted concern for ACS. As such, the patient was placed on a heparin drip and transferred by ambulance to a cardiac cath-capable facility. Note that there is virtually no artifact in ECG #2.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content