This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In one of my classes, I ask everyone what happens if you give nitro in a paramedic school scenario without obtaining a 12 lead first.? This may be something like arranging chairs to pretend you are now in a helicopter or ambulance or even expediting specific time intervals to speed up the simulation. Prehosp Emerg Care.
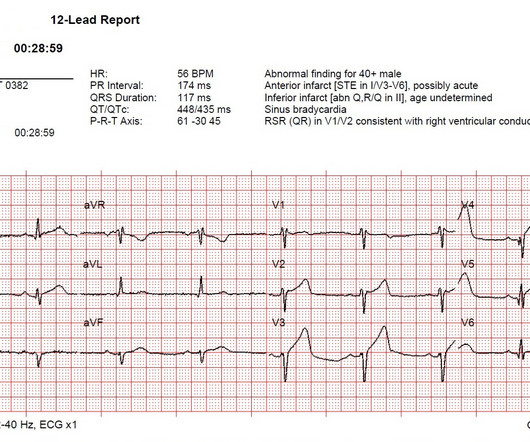
Assuming the patient has signs and symptoms of ACS, this should be an easy diagnosis. If you’re a paramedic, by obtaining a 12-lead ECG with the first set of vital signs , and not waiting until the patient is in the back of the ambulance, it gives you “another bite at the apple” before you leave the scene.
However, while LSBs have historically been used to attempt spinal immobilization, SMR may be achieved using a scoop stretcher, vacuum splint, ambulance cot, or other similar device to which a patient is safely secured. Both terms refer to the same concept — minimizing unwanted movement of the potentially injured spine.
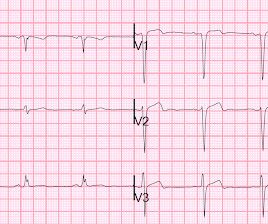
Serial ECGs demonstrated dynamic changes diagnostic of ACS (transient STEMI) 4. Even after STEMI (if reperfused, with small amount of myocardium infarcted), and even when the ECG is diagnostic of ACS (as it was the next day), the simultaneous echocardiogram may be normal. Learning Points 1. This was diagnosed as a NonSTEMI.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review provided by Dr. Steve Smith [link] @SmithECGblog A 72 y/o Male experiences a syncopal episode while seated. Attending crews then brought the stretcher close and further assisted him to a reclined position of comfort. Hospital transport was unremarkable.
Grabbing a pristine white table napkin to apply pressure to the wound, Ranulf’s class teacher and expedition leader called the ambulance as chaos descended on the restaurant. Tarquin screamed and pulled the knife straight back out, but blood started to spurt from the decent-sized incision he had accidentally made. The trauma call goes out.
Pretty impressive for someone who has not yet attended med school, or even been a nurse or paramedic yet. html ) Despite an undetectable troponin and three normal EKGs, the nature of the patients symptoms and his positive cardiac history warranted concern for ACS. This interpretation was confirmed by the overreading physician.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content