This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
She was brought in by ambulance and received aspirin and nitroglycerin en route. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. This originally radiated into her left arm. From Gue at al.
Acute anterior STEMI tends to be a more difficult ECG diagnosis than acute inferior STEMI. That’s because with acute inferior STEMI there’s almost always a downsloping ST-segment in lead aVL to help shore up the diagnosis. Assuming the patient has signs and symptoms of ACS, this should be an easy diagnosis.
The ambulance report says "BP continued to drop during transport and pt remained cold and clammy." The 3 most common causes of ACS ( A cute C oronary S yndrome ) wit hout evidence of obstructive coronary disease on cath are: i ) Myocarditis ( up to 1/3 of these patients ); ii ) Takotsubo cardiomyopathy; and , iii ) MINOCA.
The nitro she took in the ambulance did not help. Patients like her are the reason we are advocating for a change in the ACS paradigm from STEMI to OMI. While she was in her bed at home, she had sudden onset of left sided chest pain that radiated to her shoulder. The pain was pleuritic, without nausea or diaphoresis.
Based on recent studies, current guidelines recommend that O2 should not be given to non-hypoxemic patients with STEMI or NSTEMI [2,3]. REBEL Cast Ep114 – High Flow O2, Suspected ACS, and Mortality? 4159 patients (10% of total population) had STEMI 30d Mortality: High O2 protocol: 8.8% Low O2 protocol: 3.1%
Serial ECGs demonstrated dynamic changes diagnostic of ACS (transient STEMI) 4. Finally, Transient STEMI should be taken emergently to the cath lab. Normalization of Diagnostic For STEMI Prehospital ECG with Nitroglycerin Therapy. During the 13 month interval, 87 patients had an initial ECG that was diagnostic for STEMI.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. looked at consecutive patients with PE, ACS, or neither. What do you think? ng/mL, BNP 2790, and lactate 3.7. Kosuge et al.
STEMI , ST-segment elevation acute myocardial infarction ). 1 Initial diagnosis of STEMI ECG Management Recommendation Level of evidence A 12-lead ECG should be interpreted immediately (within 10 minutes) at first medical contact. I B Designated PCI centres should provide angiography and reperfusion 24/7 without delay.
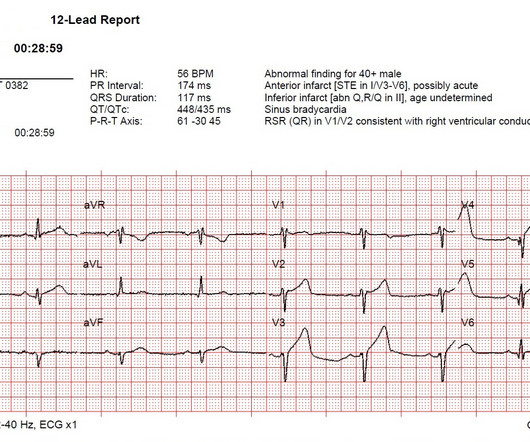
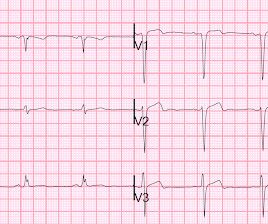
There is a very small amount of STE in some of the anterior, lateral, and inferior leads which do NOT meet STEMI criteria. One must always be careful when looking for "baseline" ECGs, because the prior ECG on file may have been during another ACS event, as this one clearly was. This ECG is highly suspicious for LAD OMI.
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. CPR was initiated immediately. It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content