This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Compensatory enlargement was defined as being present when the total coronary arterial cross-sectional area at the stenotic site was greater than that at the proximal nonstenotic site. For more on MINOCA — See My Comment in the November 16, 2023 post in Dr. Smith's ECG Blog ). As was emphasized by Dr.
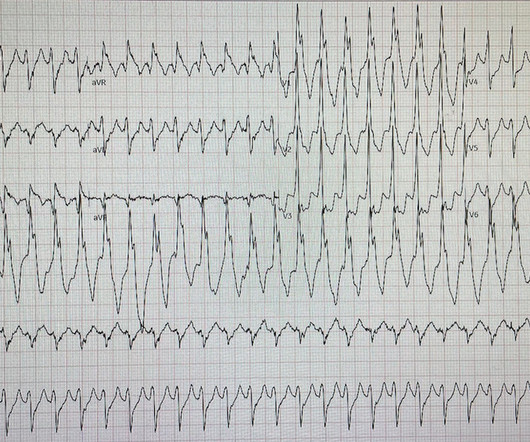
I interpreted the ECG as VT with two primary etiological possibilities: 1. Abrupt plaque ulceration of Type 1 ACS leading to VT. Readers of the Smith ECG Blog will probably recognize this a very subtle inferior OMI. The VT vs SVT with Aberrancy debate is beyond the scope of this particular blog post.
IMPRESSION: The finding of sinus bradycardia with 1st-degree AV block + marked sinus arrhythmia + the change in PR interval from beat #5-to-beat #6 — suggests a form of vagotonic block ( See My Comment in the October 9, 2020 post in Dr. Smith's ECG Blog ). Why Was Cardiac Cath Negative for Coronary Disease?
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. Essentially, we are using the troponin assay to find patients with ACO who may be benefited by coronary interventions or risk factor modification.
But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. Then assume there is ACS. As we have often emphasized on Dr. Smith's ECG Blog ( See My Comment in the March 1, 2023 post) — DSI does not indicate acute coronary occlusion! And what do you want to do?
The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). This patient is actively dying from a left main coronary artery OMI and cardiac arrest from VT/VF or PEA is imminent!
Background: Historically, we have treated acute coronary syndrome with supplemental oxygen regardless of the patient ’ s oxygen saturation. More recent evidence, however, demonstrates that too much oxygen could be harmful ( AVOID Trial ) by causing coronary vasoconstriction and increasing oxidative stress. Low O2 protocol: 3.1%
Note that as many as 7% of patients with acute coronary syndrome have chest pain reproducible on palpation [Lee, Solomon]. which reduces the pre-test probability of acute coronary syndrome by less than 30% [McGee]. It relies on an 1 mm cut point, which this blog does not favor as an approach to ECG. Back to the case. Iwaoka, R.
For the same reason, you should not delay coronary angiography because pain resolves with morphine. Smith : As Willy states, ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). But pain is a critical signal for urgency in the context of acute coronary syndrome. Worrall, C.,
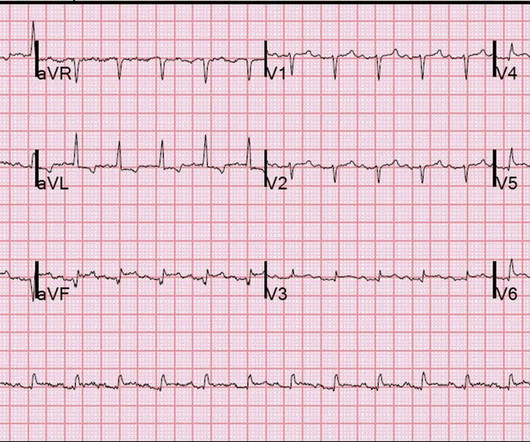
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] It’s judicious, then, to arrange for coronary angiogram.
showed that among patients with either acute coronary syndrome or acute pulmonary embolism and negative T waves in the precordial leads (V1-V4), that inverted T waves in leads III and V1 were present in only 1% of patients with acute coronary syndrome and 88% of patients with pulmonary embolism. In fact, Kosuge et al. Kosuge et al.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). ACS and hyperkalemia both have lethal downstream consequences, so it is imperative for the clinician to acclimate to the presentation, or developing, features of each. ECG's are difficult. 2] Costanzo, L.
2023 Oct 1;8(10):946-956 Question: Does the modified GRACE score incorporating continuous troponin improve ACS risk prediction? The post Modification of the GRACE Risk Score for Risk Prediction in Patients With Acute Coronary Syndromes appeared first on EMOttawa Blog. JAMA Cardiol. Methods: Retrospective.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. They too have dense white masses consistent with coronary atherosclerosis. Edited by Smith He also sent me this great case.
The ECG is just a test: a Bayesian approach to acute coronary occlusion If a patient with a recent femur fracture has sudden onset of pleuritic chest pain, shortness of breath, and hemoptysis, the D-dimer doesn’t matter: the patient’s pre-test likelihood for PE is so high that they need a CT. A Bayesian approach to acute coronary occlusion.
ACS then becomes less likely. Before the lab values returned this patient had a n emergent coronary CT angiogram done that ruled out CAD. A false positive cath lab activation is also off course acceptable for this diagnosis if you cannot get an emergent coronary CT angiogram. There are no coronary stenoses.
This was texted to me from a former resident, while working at a small rural hospital, with the statement: "I can’t convince myself of anything here, but he’s a 63-year-old guy with prior stents and a good story for ACS." We don't know if he had a stress test, a CT Coronary angiogram, or they just decided to do an angiogram.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. This is not the case.
These have all been small studies, studying very few patients with ACS, and often used final cardiology interpretation rather than patient outcome. Smith : This study had such low risk patients that not a single patient was ultimately diagnosed with ACS. It is well known that NOMI usually has a normal ECG or nonspecific ECG.
RBBB + LAFB in the setting of ACS is very bad. Some patients have baseline RBBB with LAFB, but in patients with likely ACS, these are associated with severe infarction with cardiac arrest, cardiogenic shock or impending shock. Patients with ACS and RBBB/LAFB usually have a left main vs. proximal LAD. Learning Points: 1.
ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock. Then ACS (STEMI) might be primary; this might be cardiogenic shock. One must clearly rule out these processes before jumping on the ACS diagnosis. An angiogram showed no acute coronary lesions. Are the lungs clear? The K returned at 6.9
If there were diffuse ischemic STD, with precordial STDmaxV5-6 and reciprocal STE-aVR, this would be non-specific subendocardial ischemia from ACS or supply-demand mismatch. The new ESC guidelines has for the first time merged both STEMI and non-STEMI in the same guideline because they are both on the spectrum of ACS.
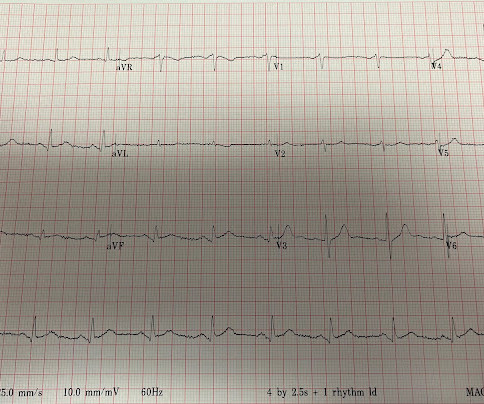
ACS would be highly unusual in a young athlete, and given the information on his race bib, one must first suspect that the abnormal ST elevation is due to demand ischemia, not ACS. The next day, and angiogram showed normal coronary arteries. Now there is much less ST segment deviation, less elevation and less depression.
Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Cardioversion will address the rhythm problem immediately, also if the chest discomfort subsides when SR is restored, ischemia from ACS becomes much less likely. In either case, prompt cardioversion is indicated.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" Furthermore, among 35 patients with acute left main coronary artery occlusion, 9 presented with RBBB (mostly with LAFB) on the admission ECG.
Now, it is true that shortly after a non-ACS cardiac arrest, there can be transient diffuse ST depression, but not ST elevation in a coronary distribution, and there should not be a wall motion abnormality. There was faint filling of the distal branches of the RCA by collaterals from the left coronary system.
There were zero patients in this study with a "normal" ECG who had any kind of ACS! Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. So this study is actually worthless.
This has been discussed many times before on this blog. In-depth discussion is beyond the scope of this blog. Serial ECGs enhance the diagnosis of acute coronary syndrome. Association of intravenous morphine use and outcomes in acute coronary syndromes: Results from the Crusade Quality Improvement Initiative. Washam, J.
I was there and said, "No, I think this is all due to severe chronic cardiomyopathy and cardiac arrest due to primary ventricular fibrillation, not due to ACS." _ Why did I say that? For this reason we did not believe this was an acute coronary event and did not activate the cath lab. So we should activate the cath lab, right?
We who know ischemic ECGs know that really when T-wave inversion is specific for coronary thrombosis that it indicates reperfusion of the artery, not active occlusion. As is often emphasized on Dr. Smith's ECG Blog — the evolution of an acute OMI is not necessarily static — but may be "dynamic". So they looked into the patient's chart.
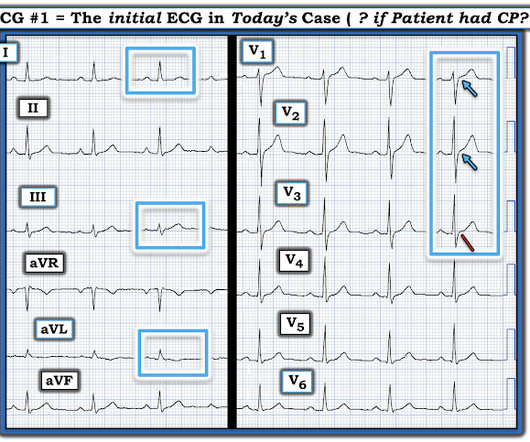
More past history: hypertension, tobacco use, coronary artery disease with two vessel PCI to the right coronary artery and circumflex artery several years prior. This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. It is unknown when this pain recurred and became constant.
A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD Although a lesion is not visible anatomically on this CT scan, coronary catheter angiography could be considered based on Cardiology evaluation." A repeat troponin returned at 0.45 CAD-RADS category 1. --No
Click here to sign up for Queen of Hearts Access Given the lack of intracranial hemorrhage, the patient was administered aspirin for suspected ACS and cardiology was consulted. Preliminary findings documented in the cath lab were “Anterior STEMI and no significant coronary artery disease.” (!!!) Version 2 = 0.0272. ng/mL and 0.10
Smith: If this is ACS (a big if), t his is just the time when one should NOT use "upstream" dual anti-platelet therapy ("upstream" means in the ED before angiography). History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Anything more on history?
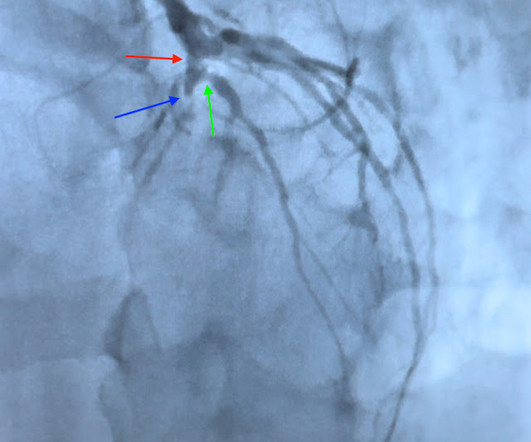
Because: 1) He has been reading this blog for a long time. The scan did not find PE, but showed evidence of coronary plaque: There are areas of dense white in the LAD (red and blue circles) and in the first diagonal (green circle). This is an RAO cranial projection of the left coronary vessels after thrombectomy and stenting.
In our opinion it should not be given in ACS unless you are committed to the cath lab. Learning Point: Any NSTEMI patient with active ongoing ACS symptoms refractory to medical management is supposed to go to the cath lab within 2 hours if available, per all guidelines in world, regardless of ECG findings. 2009;95:1701–1706.
Thus, these troponins are very concerning for ACS, and subsequent ones will probably be diagnostic of acute MI. Evidence regarding intervention to non-culprit plaques is mixed and beyond the scope of this blog post. Thus, one considers a test result that varies by 2 or less to be the same result. Heitner et al.
But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Dialysis patients have a high rate of ACS without chest pain and high rate of delayed diagnosis and delayed reperfusion 2.
But there are also hyperacute T waves (HATW) in V4-5, which exclude early repolarization and pericarditis, leaving only LAD occlusion for this patient presenting with classic symptoms of ACS. Not whether there was or was not Acute Coronary Occlusion. Not whether the ST segments met STEMI millimeter criteria. _
Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. I have posted previous such cases, but in searching my own blog, I could not find them. The ECG only tells you there is ischemia, not the etiology of it.
Despite many ECG signs of OMI being missed the door-to-cath time was still fast, because all the healthcare providers were focused on the pathology of acute coronary occlusion and not were distracted by the lack of STEMI criteria. Start using the terms acute coronary occlusion and occlusion MI.
Click here for Direct Download of the Podcast Paper: Aykan AC et al. PMID: 23102885 Aykan AC et al. appeared first on REBEL EM - Emergency Medicine Blog. Because the lungs receive 100% of cardiac output, it has been hypothesized that a lower dose of thrombolytic therapy may still be effective with a better safety profile [3][4].
The biphasic T wave is consistent with recent reperfusion of an occluded coronary artery supplying the inferior region. Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content