This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chest pain onset around 9 PM the evening prior. ECG 1 What do you think? Grines, C.
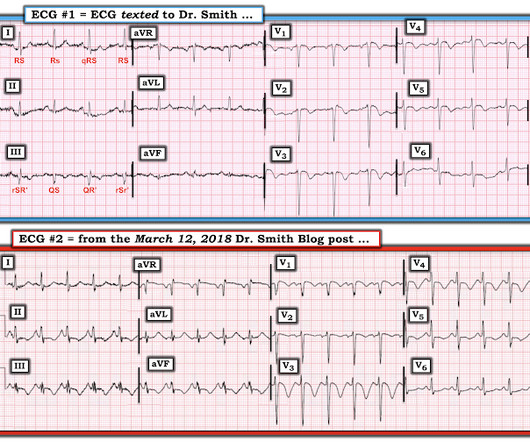
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. Challenge QUESTION: The relative change in T-QRS-D is not the only thing that changes during period of time that passed between recording of the 2 ECGs shown in Figure-1.
2024 Oct 9. You can find more details in the full blog post. There were no differences in survival (12% with IO vs 10% with IV) or neurologically intact survival (9% vs 8%). 2024 Nov 1. Restrictive vs Liberal Transfusion Strategy in Patients With Acute Brain Injury: The TRAIN Randomized Clinical Trial. doi: 10.1001/jama.2024.20424.
Learning Point: 1. As is often emphasized on Dr. Smith's ECG Blog — the evolution of an acute OMI is not necessarily static — but may be "dynamic". For examples of this phenomenon — See My Comment in the February 14, 2018 — July 21, 2020 — and December 22, 2022 posts in Dr. Smith's ECG Blog ). EMS arrived — and recorded 2 ECGs.
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. IMPRESSION: 1. hours T-wave are getting larger again The patient went for an angiogram at about 7 hours after arrival. Stroke-volume:50 ml.
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Despite not being considered in this category, opioid medications are sometimes given for ACS. Am Heart J.
Some providers were worried about ACS because of this ECG. My answer alleviated their concern for ACS and no further workup was done for ACS. 4 important features that indicate acute right hear strain: 1. looked at consecutive patients with PE, ACS, or neither. Tachycardia (or nearly) 2. Poor R-wave progression 4.
Over the last 1 week, her exertional chest pain became worse both in intensity and triggering threshold. She underwent exercise echocardiogram in mid October where she exercised for nearly 7 minutes on the standard Bruce protocol and had typical anginal pain and shortness of breath. link] Shvilkin et al. is diagnostic of cardiac memory.
This pattern occurs regardless of whether the cause is ACS (decreased supply) or any other cause of decreased supply or increased demand. You must understand that this pattern does not differentiate ACS from other causes of supply/demand mismatch. ST depression will not always be present in 9/12 leads — as is seen in Figure-1.
The pain is described as located in the midsternal area, radiating to the right arm, described as 8-9/10 and worse with deep inspirations. In the evening, he became diaphoretic and complained of 9/10 continuous chest pain. Today’s case provides perhaps the best example of s erial E CG e volution of this elusive entity.
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chest pain. On review of systems the patient reported back pain for approximately 1 week which he was treating with NSAIDs with minimal relief. 15-9/6/2017 ). His first troponin T then resulted elevated at 0.19
This ECG is quite obvious for long-time readers, and you may think this far too easy to be presented on this blog. mm in just one lead V7-9), but as far as I can tell all of these documents specifically avoid calling this condition STEMI and specifically avoid using any terminology similar to "STEMI equivalent."
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. mm of ST segment elevation, V2 and V3 have 1 mm of elevation, v4 has 2 mm of elevation and v5 around 1.5 Learning Points: 1. What do you think? V1 has 0.5
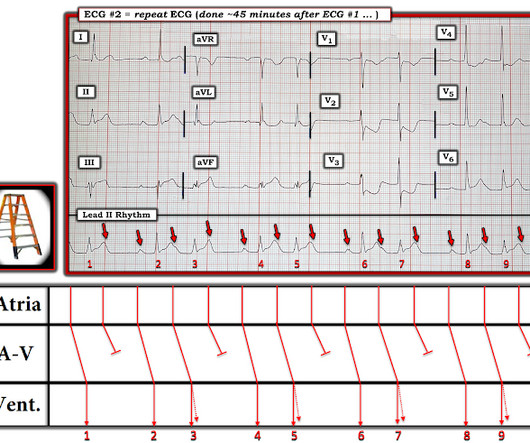
Obvious STEMI(+) OMI of inferior, posterior, and lateral walls, now with likely 2nd degree heart block type 1 (Wenckebach). STD maximal in V1-V4, without a QRS abnormality causing it, and in the setting of ACS symptoms, is posterior OMI until proven otherwise. In Figure-1 — The ST-T wave abnormality in lead V2 of ECG #1 is obvious.
There are two main etiologies of ischemic ST-depression: 1) subendocardial ischemia 2) reciprocal to ST-elevation in an opposite wall Here there are distinct R-waves with marked ST-depression throughout most of the precordium. Tips for recognizing Acute Posterior STEMI: 1. References: 1. This can help in confirmation.
Moreover , the patient has ongoing symptoms and has an unexplained elevated troponin, so she is having an MI and the only question is whether it is type 1 or type 2 due to hypertension. Case continued She was loaded with aspirin 325 mg, and repeat troponin drawn around the time of EKG 1 resulted at 267 ng/L. At midnight.
Article: Vaeli Zadeh A, Wong A, Crawford AC, Collado E, Larned JM. Guideline-based and restricted fluid resuscitation strategy in sepsis patients with heart failure: A systematic review and meta-analysis [published online ahead of print, 2023 Aug 9]. References: Vaeli Zadeh A, Wong A, Crawford AC, Collado E, Larned JM.
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. C Examination notable for diaphoresis, 1+ bilateral lower extremity edema, regular heart rate and rhythm, and no signs of respiratory distress with normal breath sounds. looked at consecutive patients with PE, ACS, or neither.
Here they are: Learning Points: 1. 7 These 3 studies, as well as 1 smaller meta-analysis, 6 and another small study, 8 make it clear that troponin is associated with increased severity and mortality in COVID when adjusted for multiple other variables. Am J Med [Internet] 2017;130(12):1431–9.e4. Available from: [link] 9.
A 40-something male presented with dyspnea and left arm numbness, and perhaps some chest tightness, for 11/2 hours. Note baseline wander in lead aVL of ECG #1. Here is his triage ECG: There is massive STE in V3-V6, and also STE in II, III, aVF. Therefore this is " Transient ST Elevation Unstable Angina." Why is this important?
Previously, I wrote a blog on pre-oxygenation, referencing my personal “weapon of choice” as chosen from the 7 Ps of RSI. But, putting them both into one blog would make for a read far too long to maintain even my attention span (which honestly is pretty short). Why is Physiologic Optimization Important?
1 His description of cases of life-threatening infections in the perineal, genital or perianal regions were thought to be idiopathic in previously healthy men. 3-5 Fournier gangrene is a type of necrotizing soft tissue infection, which can be categorized into four types based on the infectious organism involved and other features (Table 1).
1 However, it is important to understand that death from hemoptysis is almost always due to hypoxia or asphyxiation (blood impedes gas exchange in the lungs, typically because of bleeding from high-pressure bronchial arteries into the lungs) as opposed to hemodynamic instability. References Deshwal H, Sinha A, Mehta AC. 2023;23(1):87.
This blog post aims to help familiarise you with some of the most common reasons for prescribing antibiotics in the paediatric emergency department. Davidson L, Foley DA, Clifford P, Blyth CC, Bowen AC, Hazelton B, et al. Community-acquired pneumonia Addo-Yobo E, Anh DD, El-Sayed HF, Fox LM, Fox MP, MacLeod W, et al. Hibberd, O.;
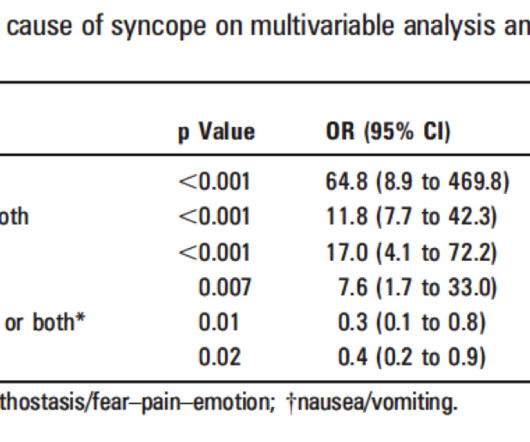
Cardiac Syncope ("True Syncope") Independent Predictors of Adverse Outcomes condensed from multiple studies 1. Palpitations preceding syncope (highest value on EGSYS score) 9. It's complicated, but they derived a score based on these variables: 1. h/o heart disease (+1) 3. Troponin greater than 99th percentile (+1) 5.
I suspect most blog readers did not struggle with this one. When the Queen has some suspicion of OMI, she asks if the patient has ACS Symptoms. The emergency physician does cautiously (correctly) note that the ECG meets STEMI criteria in V3 and V4, but goes on to document absence of ACS symptoms. Pendell Meyers , Aaron E.
The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. The top ECG is diagnostic of thrombotic type 1 OMI until proven otherwise. The RAO views above show the LAD and LCx arteries (pictures B and C, annotated in pictures E and F respectively).
1:45, case start To orient you to this screen, the top is obviously ECG waveforms. 1:51, diagnostic RCA angiography At this point, the patient very clearly has a diagnosis of OMI, especially since we visualized embolism within the PDA. & Falk, E. Papadopoulou, E., link] Falk, E., Bossone, E., Sharkey, S.,
ED Evaluation Transport to the ED from the refugee reception center takes 1 hour. g/dL, thrombocytopenia of 96 10 9 /L, prothrombin time (PT) of 16.1 1 By the end of 2023, 117.3 million people had been forcibly displaced, representing 1 in 69 individuals or 1.5% seconds (normal 30-40 seconds), creatinine of 3.11
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




























Let's personalize your content