This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
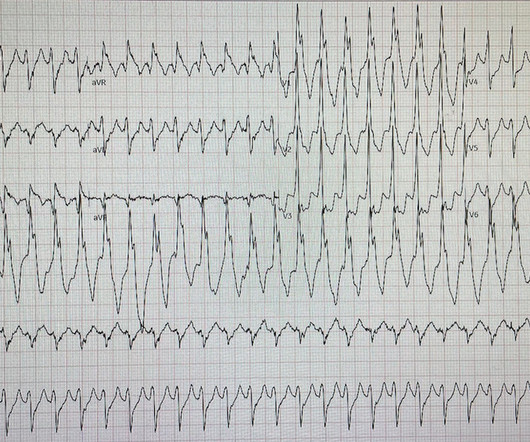
David Didlake EMT-P, RN, ACNP @DidlakeDW An adult male self-presented to the ED with palpitations and the following ECG. I interpreted the ECG as VT with two primary etiological possibilities: 1. Abrupt plaque ulceration of Type 1 ACS leading to VT. The patient was very uncomfortable, dyspneic, and displayed an SpO2 90% on RA.
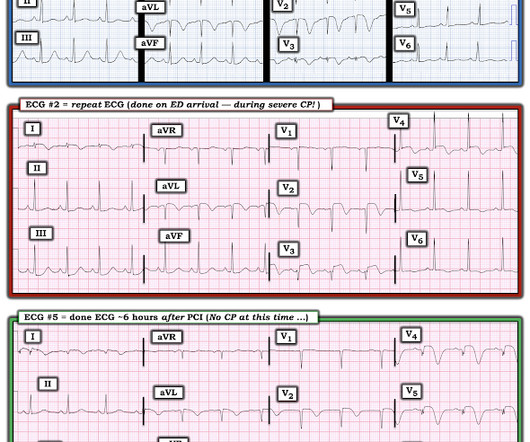
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
Full blog post here. European Journal of Internal Medicine , [link] You can listen to my 27-minute rant on Youtube here: [link] This multinational trial looked at a three-pronged diagnostic protocol in the ED for adults with suspected acute aortic syndromes. If you could achieve this process in your ED – then great.
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. Type 2 MI is common in the ED and can result from vigorous exercise (common in athletes after marathons), sepsis, trauma and tachydysrhythmias including SVT.
The patient was brought to the ED and had this ECG recorded: What do you think? Then assume there is ACS. As we have often emphasized on Dr. Smith's ECG Blog ( See My Comment in the March 1, 2023 post) — DSI does not indicate acute coronary occlusion! After 1 mg of epinephrine they achieved ROSC. sodium bicarbonate.
However, many institutions’ surgical teams still require or request a formal study over a bedside exam, likely due to a lack of confidence in the accuracy of POCUS, resulting in longer ED stays. ACS surgeons appeared to select surgery as their initial choice substantially more frequently than other subspecialties.
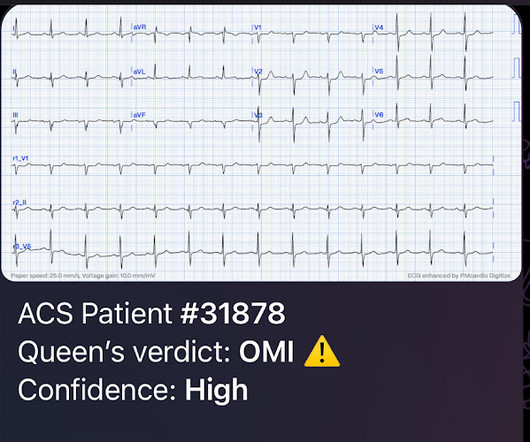
But this time the Queen gets it wrong (thinks it is not OMI): There were runs of VT: Tha patient arrived in profound shock and had an ED ECG: Now there is some evolution to include the ST elevation (rather than ST depression) in V4-V6. RBBB + LAFB in the setting of ACS is very bad. Posterior and high lateral OMI. Learning Points: 1.
showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS. In this study, (quote) "negative T waves in leads III and V 1 were observed in only 1% of patients with ACS compared with 88% of patients with Acute PE (p less than 0.001).
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). ACS and hyperkalemia both have lethal downstream consequences, so it is imperative for the clinician to acclimate to the presentation, or developing, features of each. ECG's are difficult. link] [1] Zachary et al.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing?
Cardiology consult note written around that time documents that "Pain improved with NTG, morphine in ED but still present." It relies on an 1 mm cut point, which this blog does not favor as an approach to ECG. We therefore need to assume and rule "out" ACS — more than having to rule it "in". Back to the case.
The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). Those who make it to the ED usually have transient occlusions with reperfusion.
The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. Smith : As Willy states, ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). She contacted her neighbor, a nurse, for help. The case continues.
You can find more details in the full blog post. PECARN looks at probiotics for toddlers diarrhea… Schnadower D, Tarr PI, Casper TC, Gorelick MH, Dean JM, O’Connell KJ, Mahajan P, Levine AC, Bhatt SR, Roskind CG, Powell EC, Rogers AJ, Vance C, Sapien RE, Olsen CS, Metheney M, Dickey VP, Hall-Moore C, Freedman SB.
The ECG’s were sent to the PCI center, and the providers in the respective ED identified the T wave characteristics mentioned above. From Smith ECG Blog LCx occlusion There is aVR STE with broad STD, appreciable in both Leads II and V5. Chou’s Electrocardiography in Clinical Practice (6th ed). link] [1] Mirand, D.
The person I was texting knows implicitly based on our experience together that I mean "Definite posterior OMI, assuming the patient's clinical presentation is consistent with ACS." The interventional cardiologist then canceled the activation and returned the patient to the ED without doing an angiogram ("Not a STEMI").
Here is the first ED ECG recorded, now pain free after sublingual Nitro: There is what appears to be a reperfusion T-wave in I and aVL. As is often emphasized on Dr. Smith's ECG Blog — the evolution of an acute OMI is not necessarily static — but may be "dynamic". So they looked into the patient's chart.
[link] Case continued She arrived in the ED and here is the first ED ECG. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. I don't know if her pain was getting better or not.
Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Cardioversion will address the rhythm problem immediately, also if the chest discomfort subsides when SR is restored, ischemia from ACS becomes much less likely. This patient presented to the ED “after a couple of days of chest discomfort”.
Written by Jesse McLaren A 75 year-old patient with diabetes and end stage renal disease was sent to the ED after dialysis for three days of nausea, vomiting, loose stool, lightheadedness and fatigue. But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. Below is the 15 lead ECG.
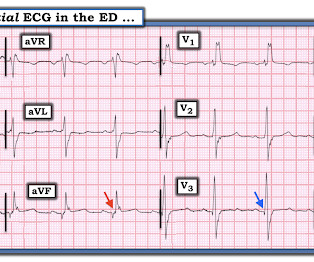
There were zero patients in this study with a "normal" ECG who had any kind of ACS! Figure-1: I've labeled the initial ECG in the ED. KEY Point: All patients who present to the ED for new CP should promptly have a triage ECG recorded, that is then immediately interpreted by the ED physician.
This is acute ACS, but it almost always seen in a pain free state. An ED ECG, if recorded with pain, should show LAD OMI. That said — severe chest pain was present at the time the patient arrived in the ED ( corresponding to the time ECG #2 was recorded ).
Prior episodes had simply resolved after brief symptoms, but the current episode had lasted for 2 hours without improvement, so she presented to the ED. At triage she stated her pain is still persistent, but it is mildly improved compared to when she decided to come to the ED. No diaphoresis or vomiting.
Because there was proven thrombus (ACS) but the troponin never went above the 99% reference range (and therefore cannot be called MI -- definition of MI requires rise and/or fall of troponin with at least one value above the 99% reference range), this is UNSTABLE ANGINA with ST Elevation. A picture is worth 1,000 words.
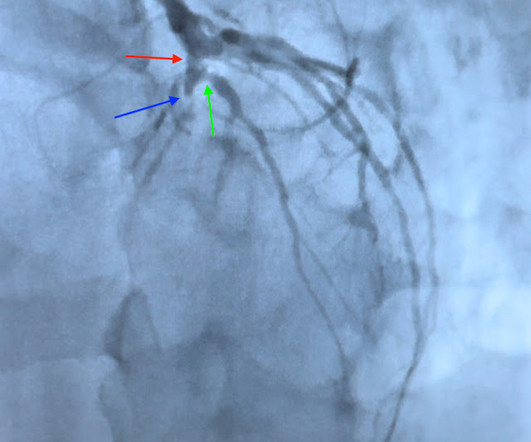
Because: 1) He has been reading this blog for a long time. He sent the patient to the ED for further evaluation. A chest x-ray in the ED found bilateral pleural effusions. The patient was admitted from the ED and finally had an angiogram the next morning: Angiogram : Image 1: This is the LAO caudal, or spider projection.
A middle-aged man complained of 15 minutes of classic angina that resolved upon arrival to the ED. But it does prove that the patient has coronary disease and makes the probability that his chest pain is due to ACS very very high. Figure-1: The initial ECG that was done in the ED ( See text ).
His parent noticed a dental problem and immediately brought the patient to the ED. Rezaie, MD (Twitter: @srrezaie ) The post Rosh Review EM Scholar Monthly Question appeared first on REBEL EM - Emergency Medicine Blog. The patient was walking his dog when it ran after a squirrel. The physical exam is shown below. Dent Traumatol.
He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines. Here is the initial ED ECG. What do you think? Rhythm : Residents asked me why it is not VT. The QRS is extremely wide.
EKG on arrival to the ED is shown below: What do you think? Click here to sign up for Queen of Hearts Access Given the lack of intracranial hemorrhage, the patient was administered aspirin for suspected ACS and cardiology was consulted. or basilar ischemia. However, T waves do not appear to be hyperacute or hyperkalemic.
Moreover, the Queen is only supposed to be used with a high pretest probability of ACS/OMI. The patient is a man in his 60s with established severe alcohol use disorder — and epidural abscess being treated with longterm Ciprofloxacin — who presented to the ED following a syncopal episode. Magnesium later resulted at 0.8 As per Drs.
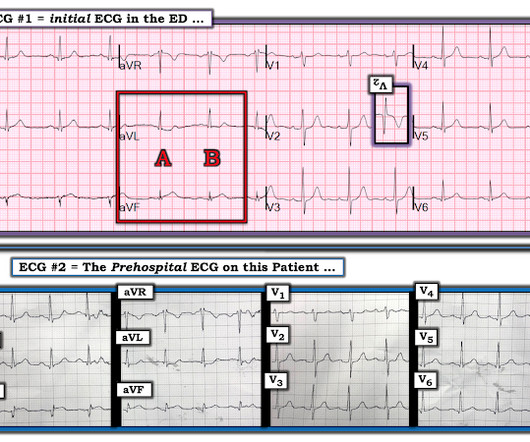
Jerry Jones commented: "Any ST depression on the ECG of a patient with chest pain credible for ACS represents a reciprocal change until proved otherwise." For clarity — I show in Figure-1 the i nitial E CG obtained in the ED ( = E CG # 1 ) — together with the p rehospital E CG that I have pieced together ( = E CG # 2 ).
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Link to abstract Link to full text 2) Use of Morphine in Non-STE-ACS is independently associated with mortality, at odds ratio of 1.4
But there are also hyperacute T waves (HATW) in V4-5, which exclude early repolarization and pericarditis, leaving only LAD occlusion for this patient presenting with classic symptoms of ACS. Chest pain still persists. Cardiology aware. Repeat troponin ordered 0630: lab called for high troponin 3900.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. In our opinion it should not be given in ACS unless you are committed to the cath lab.
Because the most severe LAD OMIs can cause ischemic failure of the RBB and LAF, any patient with ACS symptoms and new RBBB and LAFB with any concordant STE has LAD OMI until proven otherwise. In EMS2 ECG, the T waves in V5 is possibly hyperacute. So the cath lab was activated.
Here was his initial ED ECG: There is atrial fibrillation with a rapid ventricular response. Does this patient have ACS? He did not have ACS. The remainder were due to other etiologies, (including NonSTEMI ACS). But approximately 50% were due to non-ACS etiologies. A middle-aged male had a V Fib arrest.
Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. Here is the ED ECG on arrival: Less STE/STD Provider's Clinical Impression: "findings concerning for myocardial infarction, likely proximal LAD or Left main."
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Around 19 hours later, he experienced the same pain, which prompted his presentation to the ED.
The Queen of Hearts agrees: Here the Queen explains why: However, it was not interpreted correctly by the providers: ED interpretation of ECG: "paced rhythm, LBBB but no STEMI pattern." The cath report showed: Significant stenosis with subtotal occlusion (99%) in the prox to mid Lcx, culprit of ACS, TIMI flow 1.
Submitted by Dr. George Mastoras (Twitter @georgemastoras), written by Jesse McLaren It’s a busy day in the ED when you’re sent another ECG to sign off from a patient at triage. Whereas SCAD is found in ~1-4% of all angiograms performed for ACS — this percentage increases to over 30% in middle-aged women.
Smith: If this is ACS (a big if), t his is just the time when one should NOT use "upstream" dual anti-platelet therapy ("upstream" means in the ED before angiography). History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Anything more on history?
The machine indicated STEMI (but it barely meets STEMI criteria, if at all) and the patient was brought to the ED: On arrival 20 minutes later the pain had reduced to 1/10 after aspirin, and the patient had repeat ECG at triage: Now the ST segments and T waves have normalized, and the only abnormality is sinus bradycardia and loss of R waves.
This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. I was shown today’s initial ECG ( that I’ve reproduced in Figure-1 ) — knowing only that this tracing was from a patient in the ED ( therefore — a patient presumably with some kind of chest discomfort, albeit of unstated duration and severity ).
Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion. Figure 2-1 The V1 / V2 leads were appropriately placed in this circumstance, and dedicated followers of the Smith ECG Blog will instantly recognize the problem at hand. 2] Surawicz, B.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content