This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). ACS and hyperkalemia both have lethal downstream consequences, so it is imperative for the clinician to acclimate to the presentation, or developing, features of each. ECG's are difficult. link] [1] Zachary et al.
Case 1: Case 2: Case 3: Triage ECGs labeled ‘normal’ There have been a number of small studies suggesting that triage ECGs labeled ‘normal’ are unlikely to have clinical significance, and therefore that emergency physicians should not be interrupted to interpret them, and that such patients can safely wait to be seen.
He presented to the EmergencyDepartment with a blood pressure of 111/66 and a pulse of 117. ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock. Then ACS (STEMI) might be primary; this might be cardiogenic shock. One must clearly rule out these processes before jumping on the ACS diagnosis.
He arrived in the emergencydepartment hemodynamically stable. ACS would be highly unusual in a young athlete, and given the information on his race bib, one must first suspect that the abnormal ST elevation is due to demand ischemia, not ACS. On his bib it stated that he had a congenital heart disorder.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergencydepartment at around 3 AM complaining of chest pain onset around 9 PM the evening prior. Back to the case.
You can find more details in the full blog post. PECARN looks at probiotics for toddlers diarrhea… Schnadower D, Tarr PI, Casper TC, Gorelick MH, Dean JM, O’Connell KJ, Mahajan P, Levine AC, Bhatt SR, Roskind CG, Powell EC, Rogers AJ, Vance C, Sapien RE, Olsen CS, Metheney M, Dickey VP, Hall-Moore C, Freedman SB.
Background Information: Atrial fibrillation with rapid ventricular rate (RVR) is one of the many tachydysrhythmias we encounter in the EmergencyDepartment (ED). Amiodarone versus digoxin for acute rate control of atrial fibrillation in the emergencydepartment. Am J Emerg Med. Am J Emerg Med. 2022 Sep 7.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? The ST depressions in I and aVL have resolved.
A man in his 90s with a history of HTN, CKD, COPD, and OSA presented to the emergencydepartment after being found unresponsive at home. Vital signs were within normal limits on arrival to the EmergencyDepartment. Written by Bobby Nicholson What do you think of this “STEMI”? Blood glucose was not low at 162 mg/dL.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. Upon arrival to the emergencydepartment, a senior emergency physician looked at the ECG and said "Nothing too exciting." References: 1.
1 It is a quickly deployable and easily interpreted study that can be done in real time to guide decisions in the EmergencyDepartment. Point of care biliary ultrasound in the emergencydepartment (BUSED) predicts final surgical management decisions. and specificity of 88.0% Trauma Surg Acute Care Open.
There are greater than 2 million annual emergencydepartment visits for suspected renal colic in the US, and Ct scanning is performed for more than 90% of patients who receive a diagnosis of kidney stone. PMID: 25229916 DOI: 10.1056/NEJMoa1404446 Westphalen AC, Hsia RY, Maselli JH, Wang R, Gonzales R. N Engl J Med.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergencydepartment with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. 1] European guidelines add "regardless of biomarkers". But only 6.4%
She presented to the emergencydepartment after a couple of days of chest discomfort. Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? I have emphasized on many occasions in Dr. Smith's ECG Blog how AFlutter is by far (!) The last echocardiography 12 months ago showed HFmrEF.
, tells us that we physicians do not need to even look at this ECG until the patient is placed in a room because the computer says it is normal: Validity of Computer-interpreted “Normal” and “Otherwise Normal” ECG in EmergencyDepartment Triage Patients I reviewed this article for a different journal and recommended rejection and it was rejected.
A 41-year-old male who presents to the emergencydepartment with chest pain. The faculty physician thought this is highly likely to be ACS. Patient reports approximately 2 hours prior to arrival he developed a sharp chest pain that radiates into his left arm and left lower leg. Describes the radiating pain as numbness/tingling.
Smith: If this is ACS (a big if), t his is just the time when one should NOT use "upstream" dual anti-platelet therapy ("upstream" means in the ED before angiography). History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Anything more on history?
While in the emergencydepartment, he undergoes an additional ECG: 00:49 - Not much change Second ECG with measurements and calculations Magnified view of second ECGs measurements and calculation It is still "negative" for LAD occlusion (less than 23.4) Use caution when prescribing opioids to patients concerning for ACS.
I finished my residency of Emergency Medicine and I’m working at a great EmergencyDepartment here in Brazil. So, I'm a follower of your blog, and I think I have a interesting case that I attended yesterday." Aguiar last week: "Last year I had a couple of lessons with you while on my internship.
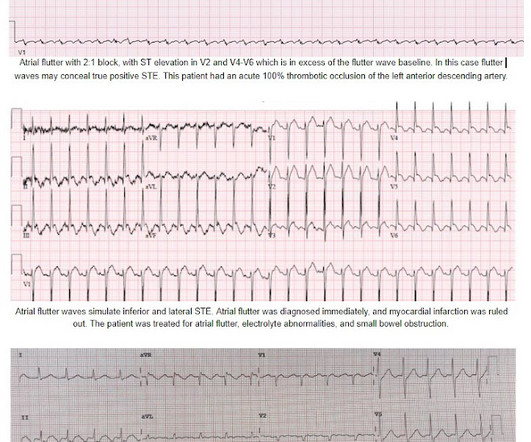
On arrival to the PCI center's EmergencyDepartment, the receiving team recorded an ECG on arrival: Persistent atrial flutter, however this time the QRS occurs on a slightly different portion of the flutter wave. The cardiologist also did not see atrial flutter, and advised giving thrombolytics for perceived "inferior STEMI."
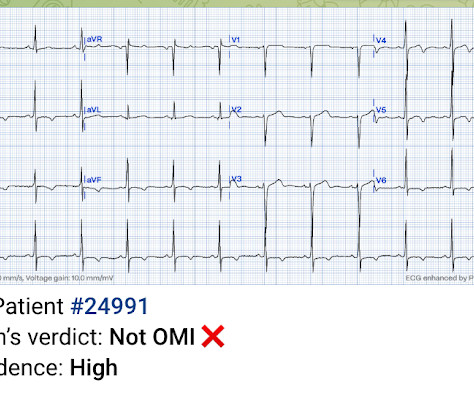
He had no symptoms of ACS. The remainder of his EmergencyDepartment stay was uneventful. Here is the clinical informaton on ECG 2: A man in his 50s presented to the EmergencyDepartment with acute chest pain that started within the past few hours. QOH: "OMI High confidence". Physician interpretation: "No STEMI."
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergencydepartment with substernal chest pain for 3 hours prior to arrival. The screening physician ordered an EKG and noted his ashen appearance and moderate distress. Triage EKG: What do you think?
52-year-old lady presents to the EmergencyDepartment with 2 hours of chest pain, palpitations & SOB. Beware of ACS presenting with atypical symptoms, including absence of chest pain. This was written by Sam Ghali ( @ EM_RESUS ), with a few edits by me. She is somewhat hypertensive, but her vital signs are otherwise normal.
She was brought to the EmergencyDepartment and this ECG was recorded while she was still feeling nauseous but denied chest pain, shortness of breath, or other symptoms: What do you think? I wouldn't activate the lab for this EKG alone, but if the patient is clinically compatible with ACS you could call a heart alert.
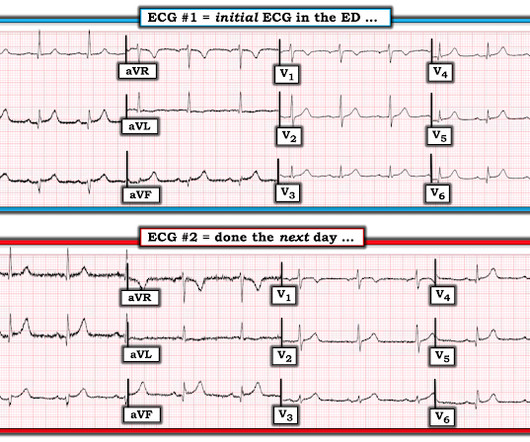
consistent with LAD occlusion) This was not recognized, repeat ECG at 69 minutes showed new Q-waves in V2-V4 that were not appreciated, and patient waited for a prolonged period in the emergencydepartment before STEMI was diagnosed. The QTc was 455 ST Elevation at 60 ms after the J-point in lead V3 = 3.0 100% LAD occlusion.
The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). The patient was rushed to the nearest emergencydepartment (non-PCI facility) for stabilization.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergencydepartment with 2 days of heavy substernal chest pain and nausea. This has been discussed many times before on this blog. In-depth discussion is beyond the scope of this blog. link] Fesmire, F.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the EmergencyDepartment via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. looked at consecutive patients with PE, ACS, or neither. What do you think? ng/mL, BNP 2790, and lactate 3.7.
Dedicated followers of the Smith ECG Blog know that the STD of true subendocardial ischemia does not localize, yet some of the examples listed below demonstrate the opposite, and were subsequently labeled “diffuse ischemia” or “generic subendocardial changes” as a diagnosis of convenience. However, the maximal STD in this case is V3.
Case submitted and written by Dr. Mazen El-Baba and Dr. Emily Austin, with edits from Jesse McLaren A 50 year-old patient presented to the EmergencyDepartment with sudden onset chest pain that began 14-hours ago. The pain improved (6/10) but is persisting, which prompted him to visit the EmergencyDepartment. Shroff, G.
Wysoki MG, Santora TA, Shah RM, Friedman AC. West J Emerg Med. Inadequate Sensitivity of Laboratory Risk Indicator to Rule Out Necrotizing Fasciitis in the EmergencyDepartment. West J Emerg Med. Image credit: Pixabay This post was peer reviewed. Click to learn more. Fournier gangrene. 2010;87(4):218-223.
A man in his 60s with a history of severe alcohol use disorder and epidural abscess on long-term ciprofloxacin presented to the emergencydepartment after an episode of syncope while standing in line at a grocery store. Moreover, the Queen is only supposed to be used with a high pretest probability of ACS/OMI.
This was sent by anonymous The patient is a 55-year-old male who presented to the emergencydepartment after approximately 3 to 4 days of intermittent central boring chest pain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin. It is unknown when this pain recurred and became constant.
Previously, I wrote a blog on pre-oxygenation, referencing my personal “weapon of choice” as chosen from the 7 Ps of RSI. But, putting them both into one blog would make for a read far too long to maintain even my attention span (which honestly is pretty short). Heffner AC, Swords DS, Neale MN, Jones AE. Crit Care Med.
But if they do present: The very common presentation of diffuse STD with reciprocal STE in aVR is NOT left main occlusion , though it might be due to sub total LM ACS, but is much more often due to non-ACS conditions, especially demand ischemia. TIMI 0/1 flow).(61,62) Knotts et al.
As recurrent ischaemia is the principle event reduced by early intervention in NSTE-ACS, these are important endpoint events occurring with delayed angiography and there is a consistent signal for harm now from two data sources.”[5] 5] This patient had ongoing chest pain, bradycardia, and no signs of reperfusion T wave inversion. Welsh et al.
Because the patient's pain had resolved completely and cardiology had declined immediate intervention, the patient was admitted but continued to board in the emergencydepartment. Approximately 4 hours after arrival, the patient was re-examined by the emergency physician. There is no age cut-off for ACS. 1] Wereski, R.,
Written by Kaley El-Arab MD, edits by Pendell Meyers and Stephen Smith A 61-year-old male with hypertension and hyperlipidemia presented to the emergencydepartment for chest tightness radiating to the back of his neck that has been intermittent for the past day or two. What do you think? Stay tuned for upcoming studies showing this.
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in EmergencyDepartment COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. of Cardiology AC, Others. Cardiac Troponin Testing in Patients with COVID-19: A Strategy for Testing and Reporting Results.
Data collected included demographics, initial rhythm, EKG, emergencydepartment (ED) CT and outcomes. We analyse disease-specific and emergency care data in order to improve the recognition of subarachnoid haemorrhage as a cause of cardiac arrest. The study population was grouped into those who did and did not have an early CT.
One of the most hair-raising presentations to the emergencydepartment (ED) can be massive hemoptysis with respiratory failure. He is the founder and host of Emergency Medicine Cases podcast and website. References Deshwal H, Sinha A, Mehta AC. The emergencydepartment evaluation and management of massive hemoptysis.
The clinicians later stated they had had no suspicion of ACS, but that the faculty wanted a troponin anyway. Design Prospective study of three independent consecutive patient populations presenting to emergencydepartments. Setting Secondary and tertiary care hospitals in the United Kingdom and United States.
This blog post aims to help familiarise you with some of the most common reasons for prescribing antibiotics in the paediatric emergencydepartment. Antibiotic Use for Common Infections in Pediatric EmergencyDepartments: A Narrative Review. Davidson L, Foley DA, Clifford P, Blyth CC, Bowen AC, Hazelton B, et al.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content