This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
VS abnormalities can drive this as well Strongly consider reversal of AC (this will typically come after control) Stopping the Bleeding PPE: these things bleed like stink. The idea behind abx is to prevent things like AOM and TSS but neither should be much of an issue with short term placement ICU Admission?
Full blog post here. PMID: 39461792 Bottom line: The WOMAN 2 trial is a large double-blind RCT that shows no benefit of TXA in the prevention of postpartum hemorrhage, which fits with all of the existing literature demonstrating no role for TXA in the management of postpartum hemorrhage. Emerg Med J. 2019 Jan;36(1):2-3. Epub 2018 Oct 25.
Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Cardioversion will address the rhythm problem immediately, also if the chest discomfort subsides when SR is restored, ischemia from ACS becomes much less likely. In either case, prompt cardioversion is indicated.
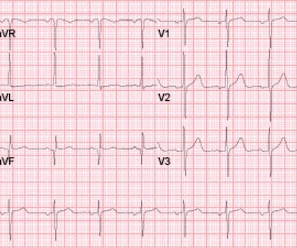
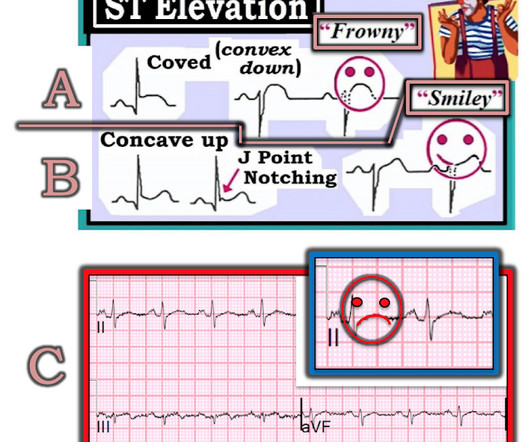
It is also true that anterior and inferior T-wave inversion could be consistent with reperfusion of a type III wraparound LAD occlusion, despite the fact that Kosuge et al showed that T-wave inversion in lead III is much more likely to be PE than ACS if your differential contains nothing else. The LV is small (underfilled) with good function.
Smith comment: We have shown that use of opiates is associated with worse outcomes in ACS: Bracey, A. The facility was not pressed to activate emergent transfer for PCI since the pain was improving and suggested we optimize pain control and admit to the Cardiac ICU. OMI is not just an ECG diagnosis.
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chest pain. The cardiologists felt that the ECG did not represent ACS, and thought it was more likely pericarditis, so they did not take him to the cath lab. in the ICU but survived with excellent function.
2 Amiodarone is commonly known for its anti-arrhythmic properties and a commonly used agent in the Intensive Care Unit (ICU). Sepsis, hyperthyroidism, dehydration, heart failure, ACS, etc). However, digoxin is known for its rate-control properties and its direct vagal effect on the atrioventricular node.
The patient was managed in the ICU and had serial troponins. An angiogram confirmed ACS as the etiology. We have addressed this issue on many occasions in Dr. Smith’s ECG Blog. It is not yet available, but this is your way to get on the list. link] Case continued This OMI was not seen by the providers. First was 2.9
I took part in her ICU care and she was extubated and stable to transfer to a stepdown unit after a few days. Patients like her are the reason we are advocating for a change in the ACS paradigm from STEMI to OMI. Her repeat ECHO showed an improving EF of 37%.
Article: Vaeli Zadeh A, Wong A, Crawford AC, Collado E, Larned JM. Secondary Outcomes: Delayed hypotension, increased ICU stay, and other relevant outcomes. References: Vaeli Zadeh A, Wong A, Crawford AC, Collado E, Larned JM. Outcomes: Primary Outcome: In-hospital mortality. 2.89, p = 0.01.
The patient was upgraded to the ICU for closer monitoring. showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS. looked at consecutive patients with PE, ACS, or neither. Kosuge et al. Witting et al. of controls.
Moreover, the Queen is only supposed to be used with a high pretest probability of ACS/OMI. The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course. We just finished training version 2 with some cases of hypokalemia, so that is in the future.
An example using a real case I had while on call in the ICU: A 61-year-old female had a post-induction arrest on the wards/hospital telemetry floor after being intubated for airway protection. PMID: 30060961 Koller AC, et al. In a PCAC 1 or 2, we may prioritize a cath and tolerate a couple hours without ICU Neuroresuscitation.
References Deshwal H, Sinha A, Mehta AC. EMCrit blog website. If it is determined that the bleeding originates from one lung it is recommended to position the patient in lateral decubitus with the bleeding lung down to avoid contamination of the contralateral lung. Life-threatening hemoptysis. Semin Respir Crit Care Med. J Emerg Med.
She did not receive any opioids (which would mask her pain without affecting any underlying ACS). If for some reason the angiogram is delayed, they should receive maximal medical therapy in an ICU setting with continuous 12-lead ST segment monitoring under the close attention of a practitioner with advanced ECG interpretation training.
Paper: Alwang AK, Law AC, Klings ES, Cohen RT, Bosch NA. The characteristics that were significantly different between the LR and NS exposure groups race, organ dysfunction at presentation, ICU admission, hemoglobin SS genotype, discharge year, and hydroxyurea use were appropriately included as confounders in the TMLE analysis.
84 All patients with severe malaria need inpatient admission, ideally to the intensive care unit (ICU). World Bank Blogs. link] Hummell AC, Cummings M. Severe malaria is typically caused by P. Uncomplicated malaria patients who are able to access prescription medication can be discharged home. Int J Equity Health. 2017;16(1):5.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content