This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
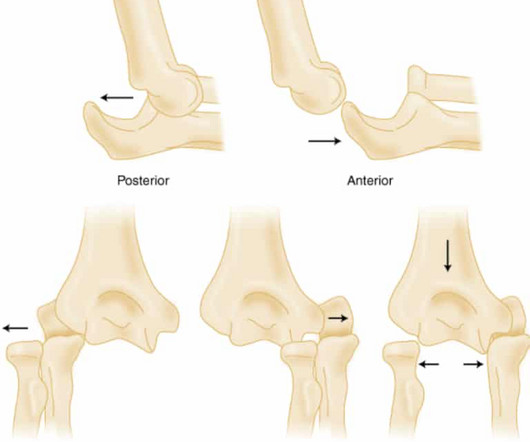
Elbow Dislocation Definition: Disarticulation of the proximal radius & ulna bones from the humerus Epidemiology: Incidence Second most common joint dislocation (after shoulder) in adults Most commonly dislocated joint in children Accounts for 10-25% of all injuries to the elbow ( Cohen 1998 ) Posterolateral is the most common type of dislocation (..)
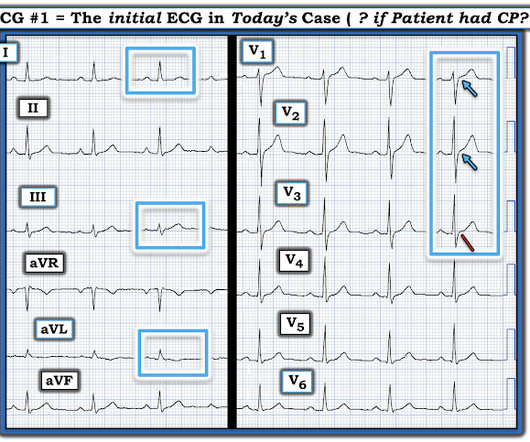
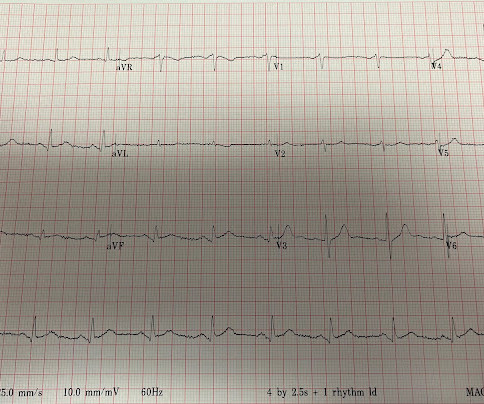
For more on MINOCA — See My Comment in the November 16, 2023 post in Dr. Smith's ECG Blog ). Review of the 2 ECGs in today's case is insightful ( Figure-1 ): The initial ECG shows sinus rhythm, LAHB and meets Peguero Criteria for LVH ( See My Comment in the August 15, 2022 post of Dr. Smith's ECG Blog for more on LVH criteria ).
Brief aside: "Early repolarization" is a frequently proclaimed and poorly understood electrocardiographic phenomenon which mostly serves to reassure clinicians that not all ST elevations are ischemic (something readers of this blog know well). It relies on an 1 mm cut point, which this blog does not favor as an approach to ECG.
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. If the patient continues to have symptoms concerning for ACS, troponin testing should be pursued. SVT is not a presenting dysrhythmia consistent w/ ACS.
Then assume there is ACS. As we have often emphasized on Dr. Smith's ECG Blog ( See My Comment in the March 1, 2023 post) — DSI does not indicate acute coronary occlusion! The ST depression usually resolves, or is clearly resolving (getting much better). This may or may not be true, but it should give you pause.
Full blog post here. Welcome to the first episode of the Broomedocs podcast for 2025. Justin and I are back for more nerdy goodness to make you smarter in the Resus room, or at a pub trivia night more likley… wether it is about salt correction, dissection or infection we can help you out! Listen in and learn! Emerg Med J.
REBEL Cast Ep114 – High Flow O2, Suspected ACS, and Mortality? PMID: 33653685 Clinical Question: Is there an association between high flow supplementary oxygen and 30-day mortality in patients presenting with a suspected acute coronary syndrome (ACS)? Click here for Direct Download of the Podcast Paper: Stewart, RAH et al.
As per my review of this subject ( Check out My Comment at the bottom of the page in the November 16, 2023 post in Dr. Smith's ECG Blog ) — the 3 most common Causes of ACS ( A cute C oronary S yndrome ) with a "negative" cath are: i ) Myocarditis; ii ) Takotsubo cardiomyopathy; and , iii ) MINOCA.
ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock. Then ACS (STEMI) might be primary; this might be cardiogenic shock. One must clearly rule out these processes before jumping on the ACS diagnosis. Are the lungs clear? Is the patient cool and pale? Large volume fluid resuscitation was undertaken.
The patient has active chest pain, so if these are abnormally large T-waves This link shows 13 blog posts of Posterior Reperfusion T-waves. Comment : ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). But it certainly shows no sign of OMI. Or does it?
showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS. In this study, (quote) "negative T waves in leads III and V 1 were observed in only 1% of patients with ACS compared with 88% of patients with Acute PE (p less than 0.001).
These have all been small studies, studying very few patients with ACS, and often used final cardiology interpretation rather than patient outcome. Smith : This study had such low risk patients that not a single patient was ultimately diagnosed with ACS. It is well known that NOMI usually has a normal ECG or nonspecific ECG.
RBBB + LAFB in the setting of ACS is very bad. Some patients have baseline RBBB with LAFB, but in patients with likely ACS, these are associated with severe infarction with cardiac arrest, cardiogenic shock or impending shock. Patients with ACS and RBBB/LAFB usually have a left main vs. proximal LAD. There is STE in aVR.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). ACE inhibitors, or potassium-sparing diuretics), are particularly susceptible. In the case of ACS, the ECG can rapidly change from this. Past medical history included HTN, HLD, and MI 10 years prior.
Smith : As Willy states, ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). Smith : As Willy states, ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). So I would be worried about inferior OMI. At midnight.
This was texted to me from a former resident, while working at a small rural hospital, with the statement: "I can’t convince myself of anything here, but he’s a 63-year-old guy with prior stents and a good story for ACS." Thank you for your work with the artificial intelligence and the blog to make people better at this.
The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). sepsis, anemia, hypoxemia, severe hypotension etc., Unless some LMCA flow is restored he will not survive.
A healthy 45-year-old female presented with chest pain, with normal vitals. The computer interpretation was “ST elevation, consider early repolarization, pericarditis or injury.” What do you think? There’s normal sinus rhythm, normal conduction, borderline right axis, and normal voltages. There’s TWI in aVL but this is concordant to its QRS.
You can find more details in the full blog post. PECARN looks at probiotics for toddlers diarrhea… Schnadower D, Tarr PI, Casper TC, Gorelick MH, Dean JM, O’Connell KJ, Mahajan P, Levine AC, Bhatt SR, Roskind CG, Powell EC, Rogers AJ, Vance C, Sapien RE, Olsen CS, Metheney M, Dickey VP, Hall-Moore C, Freedman SB.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? The ST depressions in I and aVL have resolved.
Dedicated followers of the Smith ECG Blog know that the STD of true subendocardial ischemia does not localize, yet some of the examples listed below demonstrate the opposite, and were subsequently labeled “diffuse ischemia” or “generic subendocardial changes” as a diagnosis of convenience. Here is the time-zero ECG (0939 hours).
ACS then becomes less likely. Keep an eye on the blog as an OMI QUIZ soon will be published where you test yourself vs the Queen! On arrival patient was slightly tachycardic. HR about 90-100/min. Other vital signs normal. Hand held echo showed overall ejection fraction being normal. With normal EF the tachycardia is not compensatory.
ACS would be highly unusual in a young athlete, and given the information on his race bib, one must first suspect that the abnormal ST elevation is due to demand ischemia, not ACS. His initial ECG is shown here. A bedside echo performed by the emergency physician showed no wall motion abnormality and confirmed LVH.
VS abnormalities can drive this as well Strongly consider reversal of AC (this will typically come after control) Stopping the Bleeding PPE: these things bleed like stink. Rezaie, MD (Twitter/X: @srrezaie ) The post REBEL Core Cast 123.0 – Posterior Epistaxis appeared first on REBEL EM - Emergency Medicine Blog.
Because there was proven thrombus (ACS) but the troponin never went above the 99% reference range (and therefore cannot be called MI -- definition of MI requires rise and/or fall of troponin with at least one value above the 99% reference range), this is UNSTABLE ANGINA with ST Elevation. Fortunately, that is exactly what happened.
If there were diffuse ischemic STD, with precordial STDmaxV5-6 and reciprocal STE-aVR, this would be non-specific subendocardial ischemia from ACS or supply-demand mismatch. The new ESC guidelines has for the first time merged both STEMI and non-STEMI in the same guideline because they are both on the spectrum of ACS.
But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Potassium was normal.
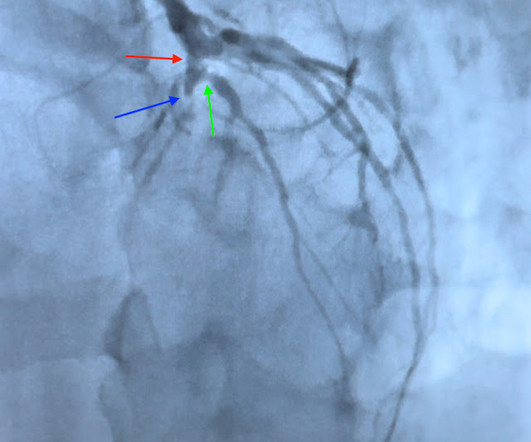
Thus, these troponins are very concerning for ACS, and subsequent ones will probably be diagnostic of acute MI. Evidence regarding intervention to non-culprit plaques is mixed and beyond the scope of this blog post. A diagnosis of "reflux" or "GERD" is never supportable without a troponin rule out. His angiogram is shown below.
The patient was thought to have low likelihood of ACS, and cardiology recommended repeat troponin, urine drug testing, and echocardiogram. At that point, cardiology elected to treat for ACS. NOTE: For review of 20 cases of "Swirl" vs Swirl "Look-Alikes" — Check out the October 15, 2022 post in Dr. Smith's ECG Blog.
Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Cardioversion will address the rhythm problem immediately, also if the chest discomfort subsides when SR is restored, ischemia from ACS becomes much less likely. In either case, prompt cardioversion is indicated.
Smith's ECG Blog — the evolution of an acute OMI is not necessarily static — but may be "dynamic". For examples of this phenomenon — See My Comment in the February 14, 2018 — July 21, 2020 — and December 22, 2022 posts in Dr. Smith's ECG Blog ). The emergency physician was skeptical and believed the ECG to be a mimic, a false positive.
Click here for Direct Download of the Podcast Paper: Aykan AC et al. Because the lungs receive 100% of cardiac output, it has been hypothesized that a lower dose of thrombolytic therapy may still be effective with a better safety profile [3][4]. REBEL Cast Ep123: Reduced-Dose Systemic Peripheral Alteplase in Massive PE?
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. It is not yet available, but this is your way to get on the list. link] Case continued She arrived in the ED and here is the first ED ECG.
Article: Vaeli Zadeh A, Wong A, Crawford AC, Collado E, Larned JM. References: Vaeli Zadeh A, Wong A, Crawford AC, Collado E, Larned JM. Rezaie, MD (Twitter/X: @srrezaie ) The post Congestive Heart Failure and Sepsis: A Closer Look at Fluid Management appeared first on REBEL EM - Emergency Medicine Blog. 2.89, p = 0.01.
Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1] 1] European guidelines add "regardless of biomarkers". But only 6.4%
Click here to sign up for Queen of Hearts Access Given the lack of intracranial hemorrhage, the patient was administered aspirin for suspected ACS and cardiology was consulted. or basilar ischemia. EKG on arrival to the ED is shown below: What do you think? However, T waves do not appear to be hyperacute or hyperkalemic. Version 2 = 0.0272.
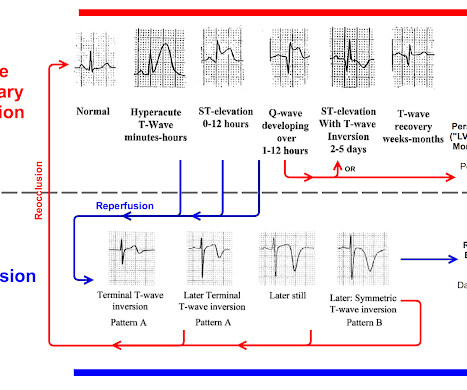
You must understand this and the dynamic nature of ACS to provide excellent care for such patients. Here is the OMI progression of ECG findings for review: You can see that OMI ECG findings must "deflate" and pass through normal or near-normal in order to get to reperfusion findings. This is termed " pseudo-normalization."
Moreover, the Queen is only supposed to be used with a high pretest probability of ACS/OMI. QTc/QUc is in the range of 630 msec. What is the most likely cause of the patient’s ECG findings, and what would be your first step in management? We just finished training version 2 with some cases of hypokalemia, so that is in the future.
This has been discussed many times before on this blog. In-depth discussion is beyond the scope of this blog. Similarly, the OMI paradigm respects ACS as a dynamic process in which ECG changes reflect the phase of myocardial injury and risk stratify which patients may benefit from emergent PCI. Leave it alone.
He had been smoking an opiate and suddenly collapsed. He was ventilated with BVM on arrival. He awoke with naloxone. This EKG was recorded as part of a standing order for critical care. He denied any CP or SOB. An EKG was repeated at 5 minutes The T-wave is less hyperacute. Maybe there is some spontaneous reperfusion? It does not radiate.
There were zero patients in this study with a "normal" ECG who had any kind of ACS! This defies all previous data on acute MI which would show that even undetectable troponins do not have a 100% negative predictive value. So this study is actually worthless. Deutch et al. West J Emerg Med 2024).
He had no symptoms of ACS. His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS." A troponin this high in a patient with no known chronic troponin elevation, and active acute ACS symptoms, has a very high likelihood of type 1 ACS regardless of the ECG.
Because: 1) He has been reading this blog for a long time. Editorial Comment: I begin my thoughts on today's Blog post with the above reflections to provide perspective for my concerns about this case. This is another case sent by the undergraduate (who is applying to med school) who works as an EKG tech.
ACS surgeons appeared to select surgery as their initial choice substantially more frequently than other subspecialties. ACS surgeons would have sent 6/43 patients for ERCP or MRCP (14%), whereas surgical oncologists would have sent a higher percentage of patients for ERCP or MRCP (7/18 or 38.9%). and specificity of 88.0%
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content