This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
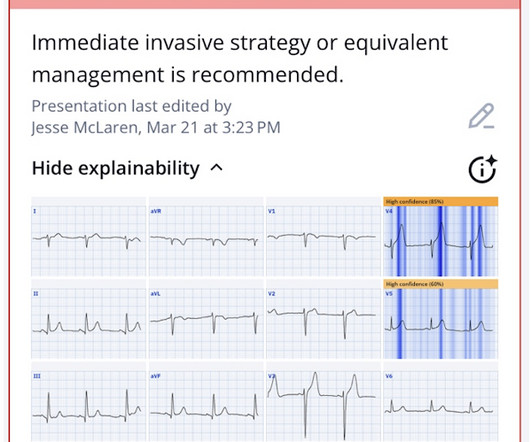
Because the most severe LAD OMIs can cause ischemic failure of the RBB and LAF, any patient with ACS symptoms and new RBBB and LAFB with any concordant STE has LAD OMI until proven otherwise. There is no recognition of STEMI equivalency in this setting in the USA guidelines currently. Long term outcome is unavailable.
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. But there are also hyperacute T waves (HATW) in V4-5, which exclude early repolarization and pericarditis, leaving only LAD occlusion for this patient presenting with classic symptoms of ACS.
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. For more on MINOCA — See My Comment in the November 16, 2023 post in Dr. Smith's ECG Blog ). He does have a recently diagnosed PE, and has not been taking his anticoagulation due to cost. He was started on nitro gtt.
These have all been small studies, studying very few patients with ACS, and often used final cardiology interpretation rather than patient outcome. Smith : This study had such low risk patients that not a single patient was ultimately diagnosed with ACS. It is well known that NOMI usually has a normal ECG or nonspecific ECG.
In this ECG Cases blog we look at 6 patients who presented with cardiorespiratory symptoms, possibly from COVID and illustrate the dangers of anchoring, being hypervigilant for cardiovascular complications, and why testing for COVID in patients being admitted for ACS is important.
He was rushed by residents into our critical care room with a diagnosis of STEMI, and they handed me this ECG: There is sinus tachycardia with ST elevation in II, III, and aVF, as well as V4-V6. At first glance, it seems the patient is having a STEMI. ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock.
Then assume there is ACS. Cardiac arrest #3: ST depression, Is it STEMI? As we have often emphasized on Dr. Smith's ECG Blog ( See My Comment in the March 1, 2023 post) — DSI does not indicate acute coronary occlusion! The ST depression usually resolves, or is clearly resolving (getting much better).
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. Do NOT give it unless you are committed to the cath lab!! Cath attending is aware. It is a mass delusion.
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
Based on recent studies, current guidelines recommend that O2 should not be given to non-hypoxemic patients with STEMI or NSTEMI [2,3]. REBEL Cast Ep114 – High Flow O2, Suspected ACS, and Mortality? 4159 patients (10% of total population) had STEMI 30d Mortality: High O2 protocol: 8.8% Low O2 protocol: 3.1%
If there were diffuse ischemic STD, with precordial STDmaxV5-6 and reciprocal STE-aVR, this would be non-specific subendocardial ischemia from ACS or supply-demand mismatch. So when the first troponin returned at 2,200 ng/L (normal <26 in males and <16 in females) the patient was referred to cardiology as a non-STEMI.
The person I was texting knows implicitly based on our experience together that I mean "Definite posterior OMI, assuming the patient's clinical presentation is consistent with ACS." The interventional cardiologist then canceled the activation and returned the patient to the ED without doing an angiogram ("Not a STEMI").
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Smith : As Willy states, ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC).
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? The ST depressions in I and aVL have resolved.
The patient has active chest pain, so if these are abnormally large T-waves This link shows 13 blog posts of Posterior Reperfusion T-waves. Comment : ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). Therefore, we activate the Cath Lab.
There were zero patients in this study with a "normal" ECG who had any kind of ACS! So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. Deutch et al.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. This is not unusual. Take home 1.
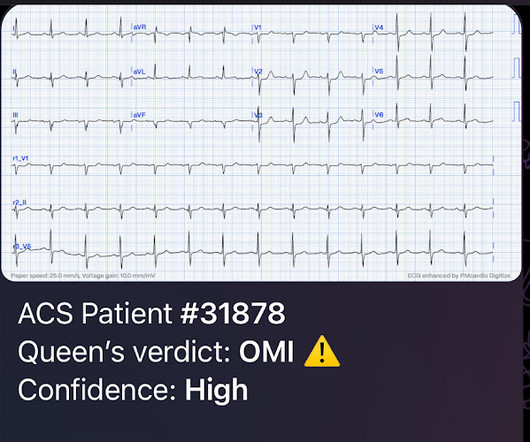
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). There is mixed overlap of ST-segment elevation (STE), ST-segment depression (STD), Hyperacute T waves (HATW), and deWinter pattern (which the ACC regards as a STEMI-equivalent but is better suited under the blanket of OMI).
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al.
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS. Kosuge et al. Witting et al.
ACS would be highly unusual in a young athlete, and given the information on his race bib, one must first suspect that the abnormal ST elevation is due to demand ischemia, not ACS. Thus, this patient had increased ST elevation (current of injury) superimposed on the ST elevation of LVH and simulating STEMI.
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). With EMS, patient had a GCS of 3 and was saturating 60% on room air. Version 2 = 0.0272.
I sent this ECG to the Queen of Hearts (PMcardio OMI), and here is the verdict: You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form Then I learned that a Code STEMI was activated for concern of anterior "STEMI" in V1-V2. High sensitivity troponin I was 23 ng/L.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. This case is an example of the steps we can all take in daily practice as the paradigm shifts from STEMI to OMI.
This has been discussed many times before on this blog. In-depth discussion is beyond the scope of this blog. The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Is there STEMI? The patient continued having chest pain. What is the rhythm? References: Ferrier, G.
Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Day 12 ECG: FINAL DIAGNOSIS: "NSTEMI" Despite the fact that his day 4 ECG easily meets STEMI criteria, the patient is diagnosed as NSTEMI. No TIMI flow was listed in the report. Am Heart J.
This is a 45 yo male who had an inferior STEMI 6 months prior, was found to have severe LAD and left main disease, and was supposed to be set up for CABG a few weeks later, but did not follow up. But it could be anterior STEMI. 40% of anterior STEMI has upward concavity in all of leads V2-V6. is likely anterior STEMI).
This ECG was read as “No STEMI” with no prior available for comparison. It is true this ECG does not meet STEMI criteria (there is 1.0 The Queen of Hearts sees it of course: Still none of these three ECGs meet STEMI criteria. Do you think we discussed this patient's 2-3 hour delay to reperfusion in our quarterly "STEMI meeting"?
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? This is the response he got: Interventionist: "No STEMI, no cath. After stabilizing the patient and recording more ECGs, he tried again: Interventionalist: "It isn't a STEMI." It is a STEMI equivalent. We don't know how many though.
This is as clear a STEMI as you can get. Now, it is true that shortly after a non-ACS cardiac arrest, there can be transient diffuse ST depression, but not ST elevation in a coronary distribution, and there should not be a wall motion abnormality. So this is classic inferoposterior STEMI on the ECG but is NOT acute coronary syndrome!
This ECG is quite obvious for long-time readers, and you may think this far too easy to be presented on this blog. Furthermore, the term "STEMI equivalent" has no reliable or definable meaning except between two practitioners who both agree on the list of entities that they believe are STEMI equivalents and can agree on how to identify it.
STEMI was activated and the patient went to Cath on arrival. From Smith ECG Blog LCx occlusion There is aVR STE with broad STD, appreciable in both Leads II and V5. Readers interested in a more robust discussion of STD vectors, and their implications in OMI, are encouraged to read this phenomenal post at the Smith ECG Blog.
He had an immediate ED ECG: There is artifact, but the findings appear to be largely gone now The diagnosis is acute MI, but not STEMI. See this post on the (Five primary patterns of ischemic ST depression, without ST elevation) Because of the dynamic ACS, we activated the cath lab in the middle of the night.
You can see how V1, V2, aVR, and V4R would have ST elevation in either a right ventricular STEMI or with a septal STEMI, and how lateral leads, and even posterior leads, would have reciprocal ST depression. of patients with anterior STEMI, ST elevation of greater than or equal to 3.0 STE in V4R is confirmatory evidence.
This patient could have very easily been overlooked, both because the ECG was STEMI negative and because the Q waves were attributed to an “old infarct”. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion. OMI or STEMI? As cardiology documented, “possible STEMI.
He has been following the blog for 4 years. The emergency physician asked the advice of Dr. Reiters because of absence of STEMI criteria. This case was sent by Dr. Jean-christophe Reiters, an interventionalist in Belgium. He has now implemented the Queen of Hearts in his hospital. He wanted to share one of the first cases.
The Queen of Hearts agrees: Here the Queen explains why: However, it was not interpreted correctly by the providers: ED interpretation of ECG: "paced rhythm, LBBB but no STEMI pattern." Most large STEMI have peak troponin I in the 20.0 There are hyperacute T-waves in V5 and V6. Next trop in AM. Peak trop 257.97 ng/mL - 80.0
He had multiple cardiovascular risk factors and the EM physician strongly suspected ACS. Over the next few hours, four other general cardiologists "signed off on the initial ECG without recognizing STEMI." Learning Points: STEMI criteria misses 25-40% of OMI, like this case for example. mm of the "required" 1.0
Thus, these troponins are very concerning for ACS, and subsequent ones will probably be diagnostic of acute MI. Evidence regarding intervention to non-culprit plaques is mixed and beyond the scope of this blog post. Thus, one considers a test result that varies by 2 or less to be the same result. Heitner et al.
Because there was proven thrombus (ACS) but the troponin never went above the 99% reference range (and therefore cannot be called MI -- definition of MI requires rise and/or fall of troponin with at least one value above the 99% reference range), this is UNSTABLE ANGINA with ST Elevation. A picture is worth 1,000 words.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. His response: “subendocardial ischemia. Anything more on history? POCUS will be helpful.”
He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. Sensitivity was 87% for OMI in our validation study (it was 34% for STEMI criteria). So it can miss some OMI.
Only very slight STE which does not meet STEMI criteria at this time. I am immediately worried that this OMI will not be understood, for many reasons including lack of sufficient STE for STEMI criteria, as well as the common misunderstanding of "no reciprocal findings" which is very common with this particular pattern.
Discharge ECG showed antero-inferior reperfusion T wave inversion: Had the initial ECG been signed off as “STEMI negative” the patient could have arrested in the waiting room, with a poor cardiac and neurological outcome. For more on this topic — See discussion in the October 24, 2019 and July 31, 2018 posts in Dr. Smith's ECG Blog ).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content