

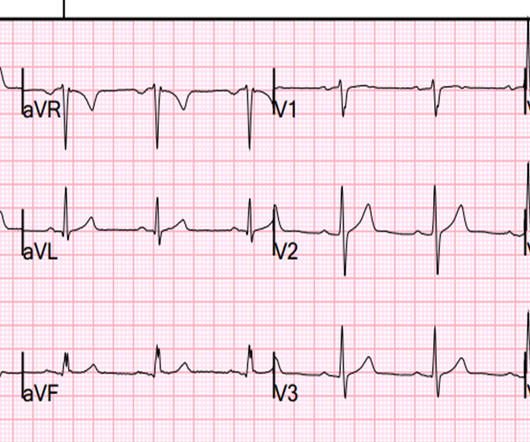
An undergraduate who is an EKG tech sees something. The computer calls it completely normal. How about the physicians?
Dr. Smith's ECG Blog
MAY 20, 2024
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chest pain, shortness of breath, and diaphoresis after consuming a large meal at noon. Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? Edited by Smith He also sent me this great case.

























Let's personalize your content