This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The 2022 American College of Cardiology (ACC) pathway provides timely guidance [1]. Intermediate-risk patients may be further stratified based on recent stress testing or coronary angiogram findings plus a modified HEART or Emergency Department Assessment of Chest Pain (EDACS) score. Time to know your hs-cTn better.
Moreover , the patient has ongoing symptoms and has an unexplained elevated troponin, so she is having an MI and the only question is whether it is type 1 or type 2 due to hypertension. Case continued She was loaded with aspirin 325 mg, and repeat troponin drawn around the time of EKG 1 resulted at 267 ng/L. At midnight.
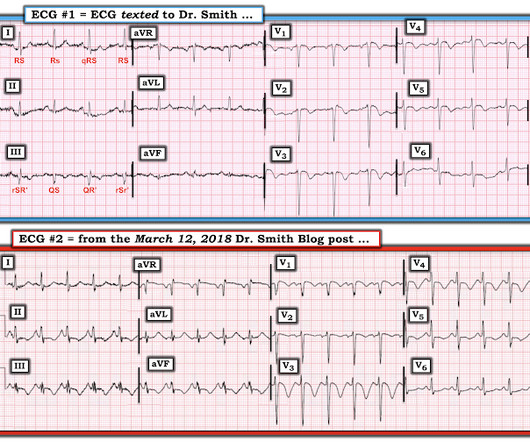
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. Challenge QUESTION: The relative change in T-QRS-D is not the only thing that changes during period of time that passed between recording of the 2 ECGs shown in Figure-1.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chest pain onset around 9 PM the evening prior. ECG 1 What do you think? Grines, C.
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. C Examination notable for diaphoresis, 1+ bilateral lower extremity edema, regular heart rate and rhythm, and no signs of respiratory distress with normal breath sounds. What do you think? In fact, Kosuge et al. Stein et al.
We who know ischemic ECGs know that really when T-wave inversion is specific for coronary thrombosis that it indicates reperfusion of the artery, not active occlusion. Learning Point: 1. For examples of such exceptions — See My Comment in the January 9, 2019 — August 22, 2020 — and June 30, 2023 posts in Dr. Smith's ECG Blog ).
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Despite not being considered in this category, opioid medications are sometimes given for ACS. Am Heart J.
This pattern occurs regardless of whether the cause is ACS (decreased supply) or any other cause of decreased supply or increased demand. You must understand that this pattern does not differentiate ACS from other causes of supply/demand mismatch. ST depression will not always be present in 9/12 leads — as is seen in Figure-1.
All patients with NSTE-ACS ( NSTEMI or unstable angina) are treated similarly with respect to anti-ischemic and anti-thrombotic drugs. Management must, however, be individualized with respect to the delay to coronary angiography (PCI). TIMI Risk Scores for NSTE-ACS (NSTEMI, UA) and STE-ACS ( STEMI ) can be calculated below.
Some providers were worried about ACS because of this ECG. My answer alleviated their concern for ACS and no further workup was done for ACS. 4 important features that indicate acute right hear strain: 1. looked at consecutive patients with PE, ACS, or neither. Tachycardia (or nearly) 2. Poor R-wave progression 4.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. mm of ST segment elevation, V2 and V3 have 1 mm of elevation, v4 has 2 mm of elevation and v5 around 1.5 What do you think? V1 has 0.5 mm of elevation.
The pain is described as located in the midsternal area, radiating to the right arm, described as 8-9/10 and worse with deep inspirations. In the evening, he became diaphoretic and complained of 9/10 continuous chest pain. If there is NO WMA, then it is not coronary occlusion, but if there IS one, then you still don't have a diagnosis.
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chest pain. On review of systems the patient reported back pain for approximately 1 week which he was treating with NSAIDs with minimal relief. 15-9/6/2017 ). His first troponin T then resulted elevated at 0.19
Most agents exhibit both vasopressor and inotropic effects (Figure 1). Below follows a drug manual for use in the CCU (coronary care unit), ICU (intensive care unit) or ER (emergency room). μg/kg/min + + + ++ Low dose dopamine stimulates D1 receptors and induces vasodilation in coronary, renal, cerebral and mesenteric vessels.
There are two main etiologies of ischemic ST-depression: 1) subendocardial ischemia 2) reciprocal to ST-elevation in an opposite wall Here there are distinct R-waves with marked ST-depression throughout most of the precordium. Tips for recognizing Acute Posterior STEMI: 1. References: 1. This can help in confirmation.
A 40-something male presented with dyspnea and left arm numbness, and perhaps some chest tightness, for 11/2 hours. E CG # 1 = the initial Triage ECG ( TOP ) — As per Dr. . = Here is his triage ECG: There is massive STE in V3-V6, and also STE in II, III, aVF. Why is this important? Mokhtari et al. JACC 2016;67:1531.
And so it is wise to look at the coronary arteries. Here they are: Learning Points: 1. This ECG certainly looks like myocarditis, and was due to myocarditis, but missing acute coronary occlusion is not acceptable. In acute MI, the T-wave is large, and the T/ST ratio is high. This is much more typical of myocarditis.
mm in just one lead V7-9), but as far as I can tell all of these documents specifically avoid calling this condition STEMI and specifically avoid using any terminology similar to "STEMI equivalent." It's an ECG manifestation of transmural MI from an occluded coronary artery registered in the ECG leads FACING the infarcted ventricular wall.
The neurologic section was divided into (1) brain oxygenation, perfusion, edema, and intracranial pressure (ICP); (2) seizures and the ictal-interictal continuum (IIC); and (3) sedation and analgesia. Reference: Hirsch KG, Abella BS, Amorim E, et al; American Heart Association, Neurocritical Care Society. 2023 Dec 1.
1 Indications for transplant include: Non-ischemic cardiomyopathy (49%) Ischemic cardiomyopathy (35%) Restrictive cardiomyopathy (4%) Retransplantation following failed prior transplant (3%) Hypertrophic cardiomyopathy (3%) Congenital heart disease (3%) Valvular cardiomyopathy (3%) The median survival after heart transplant is over 12 years.
She describes the pain as left-sided, non-radiating, and 9/10 in severity. The catheterization lab is activated, but catheterization shows no coronary artery occlusion. A 67-year-old female with past medical history of hypertension presents with acute onset of chest pain without associated symptoms. What is the diagnosis?
1 The ED is a fast-paced environment where patient stability and life-and-limb-threatening conditions are prioritized. The pain began abruptly 1 hour ago, described as a stabbing sensation, and has occurred daily at the same time for the past week, each episode lasting about 45 minutes. Pain can be improved or exacerbated with meals.
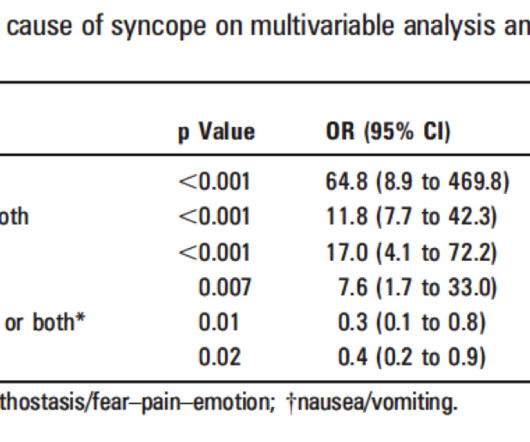
Cardiac Syncope ("True Syncope") Independent Predictors of Adverse Outcomes condensed from multiple studies 1. Palpitations preceding syncope (highest value on EGSYS score) 9. It's complicated, but they derived a score based on these variables: 1. h/o heart disease (+1) 3. Troponin greater than 99th percentile (+1) 5.
1:45, case start To orient you to this screen, the top is obviously ECG waveforms. The arterial pressure waveform is transduced using the coronary catheter. But in the case of an ostial lesion, there is little or no space between the outside of the catheter and the wall of the coronary artery.
The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. The scan showed a bicuspid aortic valve with severe stenosis and coronary artery disease. The top ECG is diagnostic of thrombotic type 1 OMI until proven otherwise.
When the Queen has some suspicion of OMI, she asks if the patient has ACS Symptoms. The emergency physician does cautiously (correctly) note that the ECG meets STEMI criteria in V3 and V4, but goes on to document absence of ACS symptoms. Pendell Meyers , Aaron E. PEARL #2: The above said Remember the rule of "N = 1".
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content