This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Encourage your ED to set up an algorithm that you can follow based on your laboratory’s assay. Low-risk patients do not routinely require stress testing in the ED. You (or someone in your department) needs to know which assay your ED has, and use the appropriate values for that assay. Otherwise, apply a simplified approach.
At the time of ED arrival he was alert, oriented, and verbalizing only a headache with a normalized BP. The ED activated trauma services, and a 12 Lead ECG was captured. This was deemed “non-specific” by the ED physicians. Thus, the ED admission ECG changes cannot be blamed on LVH. The fall was not a mechanical etiology.
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
Case: You are working a busy shift in a rural emergency department (ED) and your excellent Family Medicine trainee presents a case of a 63-year-old woman with chest pain and some intermittent radiation into the inter-scapular region. The patient has no specific risk factors for acute coronary syndrome (ACS) or dissection.
[link] Case continued She arrived in the ED and here is the first ED ECG. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. The Queen no longer thinks it is OMI.
Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Case: You are working a shift in your local community emergency department (ED) when a 47-year-old male presents with chest pain.
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. Essentially, we are using the troponin assay to find patients with ACO who may be benefited by coronary interventions or risk factor modification.
Date: January 16th, 2020 Reference: Troponin Testing and Coronary Syndrome in Geriatric Patients With Nonspecific Complaints: Are We Overtesting? Date: January 16th, 2020 Reference: Troponin Testing and Coronary Syndrome in Geriatric Patients With Nonspecific Complaints: Are We Overtesting? Reference: Wang et al.
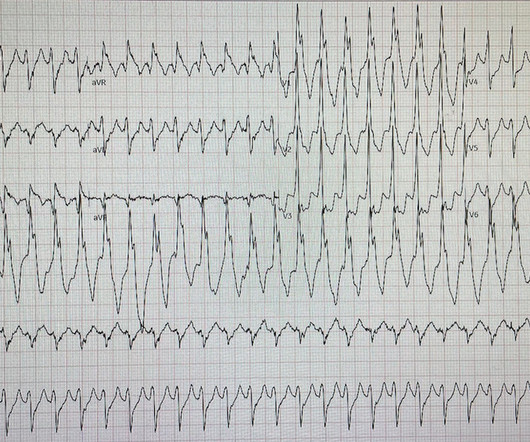
David Didlake EMT-P, RN, ACNP @DidlakeDW An adult male self-presented to the ED with palpitations and the following ECG. I interpreted the ECG as VT with two primary etiological possibilities: 1. Abrupt plaque ulceration of Type 1 ACS leading to VT. The patient was very uncomfortable, dyspneic, and displayed an SpO2 90% on RA.
The patient was brought to the ED and had this ECG recorded: What do you think? But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. Then assume there is ACS. Smith's ECG Blog ( See My Comment in the March 1, 2023 post) — DSI does not indicate acute coronary occlusion!
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (ret) @DidlakeDW Expert commentary and peer review by Dr. Steve Smith [link] @smithECGBlog A 57 y/o Female with PMHx HTN, HLD, DM, and current use of tobacco products, presented to the ED with chest discomfort. It’s judicious, then, to arrange for coronary angiogram.
Although the attending crews did not consider the ECG pathognomonic for occlusive thrombosis, they nonetheless considered the patient high-risk for ACS and implored him to reconsider. One cannot rely on this feature as a means of detecting changes – subtle, or dramatic – for volatile occlusive coronary thrombus.
He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP). She arrives in the emergency department (ED) with decreased level of consciousness and shock.
The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). This patient is actively dying from a left main coronary artery OMI and cardiac arrest from VT/VF or PEA is imminent!
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. They too have dense white masses consistent with coronary atherosclerosis. Edited by Smith He also sent me this great case.
showed that among patients with either acute coronary syndrome or acute pulmonary embolism and negative T waves in the precordial leads (V1-V4), that inverted T waves in leads III and V1 were present in only 1% of patients with acute coronary syndrome and 88% of patients with pulmonary embolism. In fact, Kosuge et al. Kosuge et al.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). ACS and hyperkalemia both have lethal downstream consequences, so it is imperative for the clinician to acclimate to the presentation, or developing, features of each. ECG's are difficult. 2] Costanzo, L.
David Didlake, FF/EMT-P, AG-ACNP @DidlakeDW An elder female presented to the ED with worsening shortness of breath. She was known to have a history of poorly controlled COPD, AFib, and multivessel coronary disease. This should prompt immediate investigation into supply-demand mismatching, or ACS.
The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. For the same reason, you should not delay coronary angiography because pain resolves with morphine. But pain is a critical signal for urgency in the context of acute coronary syndrome. Mukherjee, D.,
He advises, however, recurrent syncopal episodes for the past six months, some of which have resulted in ED admission, yet no identifying mechanism could be determined. 3,4] The final 12 Lead ECG does not meet any Smith-modified Sgarbossa criteria, so the T wave signatures are characteristic of improved coronary flow, but not necessarily MI.
But this time the Queen gets it wrong (thinks it is not OMI): There were runs of VT: Tha patient arrived in profound shock and had an ED ECG: Now there is some evolution to include the ST elevation (rather than ST depression) in V4-V6. RBBB + LAFB in the setting of ACS is very bad. Posterior and high lateral OMI. Learning Points: 1.
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] It’s judicious, then, to arrange for coronary angiogram.
He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines. Here is the initial ED ECG. So a dual chamber pacer is placed with one lead through the coronary sinus to the LV.
Note that as many as 7% of patients with acute coronary syndrome have chest pain reproducible on palpation [Lee, Solomon]. which reduces the pre-test probability of acute coronary syndrome by less than 30% [McGee]. Cardiology consult note written around that time documents that "Pain improved with NTG, morphine in ED but still present."
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" Smith and Meyers answer: First , LM occlusion is uncommon in the ED because most of these die before they can get a 12-lead recorded.
There were zero patients in this study with a "normal" ECG who had any kind of ACS! Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. So this study is actually worthless.
Now, it is true that shortly after a non-ACS cardiac arrest, there can be transient diffuse ST depression, but not ST elevation in a coronary distribution, and there should not be a wall motion abnormality. There was faint filling of the distal branches of the RCA by collaterals from the left coronary system.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. This is not the case.
AEM May 2022 Guest Skeptic: Dr. Justin Morgenstern is an emergency physician and the creator of the #FOAMed project called First10EM.com Case: A 33-year-old male presents to the emergency department (ED) complaining of abdominal pain. He doesn’t have any specific symptoms today, including no fever, vomiting, diarrhea, or urinary symptoms.
More past history: hypertension, tobacco use, coronary artery disease with two vessel PCI to the right coronary artery and circumflex artery several years prior. This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. It is unknown when this pain recurred and became constant.
This post will focus on the key parts of the guideline that affect ED evaluation and management. Editorial Comment: ECPR may be considered in patients refractory to standard ACS in the right situation. Major Updates Avoid routine use of calcium in patients with cardiac arrest. COR 2a, LOE B-R. COR 1, LOE B-NR. COR 2a, LOE B-NR.
Notoriously elusive, with a high misdiagnosis rate, thoracic aortic dissection (AD) can mimic many conditions, including acute coronary syndrome (ACS, the most common), gastroesophageal reflux disease (GERD), stroke, and spinal-cord compression. In the ED, his troponin, ECG, and chest X-ray (CXR) are normal. He survives.
The machine indicated STEMI (but it barely meets STEMI criteria, if at all) and the patient was brought to the ED: On arrival 20 minutes later the pain had reduced to 1/10 after aspirin, and the patient had repeat ECG at triage: Now the ST segments and T waves have normalized, and the only abnormality is sinus bradycardia and loss of R waves.
Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Cardioversion will address the rhythm problem immediately, also if the chest discomfort subsides when SR is restored, ischemia from ACS becomes much less likely. This patient presented to the ED “after a couple of days of chest discomfort”.
1] Here is the admitting ED ECG after cancellation of Code STEMI. The patient continued to verbalize cessation of symptoms while in the ED. Cardiology admitted him for observation with plans for next-day coronary angiogram. However, in this context (i.e. V2 – in the final EMS ECG the ST segment was baseline. 1] Driver, B.
A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD Although a lesion is not visible anatomically on this CT scan, coronary catheter angiography could be considered based on Cardiology evaluation." A repeat troponin returned at 0.45 CAD-RADS category 1. --No
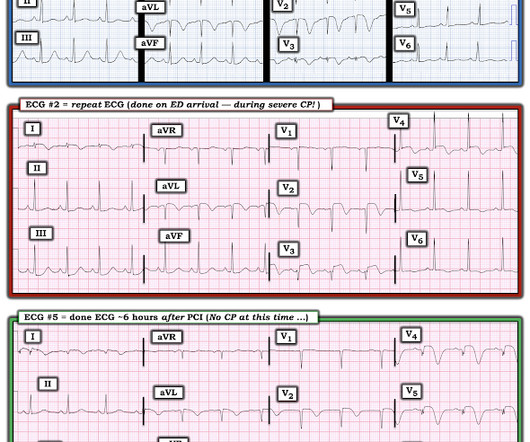
This is acute ACS, but it almost always seen in a pain free state. An ED ECG, if recorded with pain, should show LAD OMI. That said — severe chest pain was present at the time the patient arrived in the ED ( corresponding to the time ECG #2 was recorded ).
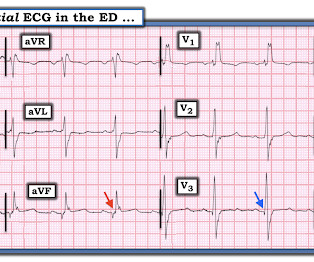
A middle-aged man complained of 15 minutes of classic angina that resolved upon arrival to the ED. But it does prove that the patient has coronary disease and makes the probability that his chest pain is due to ACS very very high. Figure-1: The initial ECG that was done in the ED ( See text ).
We who know ischemic ECGs know that really when T-wave inversion is specific for coronary thrombosis that it indicates reperfusion of the artery, not active occlusion. Here is the first ED ECG recorded, now pain free after sublingual Nitro: There is what appears to be a reperfusion T-wave in I and aVL. Some patients do this.
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Association of intravenous morphine use and outcomes in acute coronary syndromes: Results from the CRUSADE Quality Improvement Initiative.
Sent by anonymous, written by Pendell Meyers A man in his late 40s presented to the ED with concern for allergic reaction after accidentally eating a potential allergen, then developing an itchy full body rash and diarrhea. In the ED he received methylprednisolone, diphenhydramine, and epinephrine for possible anaphylaxis.
Smith: If this is ACS (a big if), t his is just the time when one should NOT use "upstream" dual anti-platelet therapy ("upstream" means in the ED before angiography). History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Anything more on history?
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. In our opinion it should not be given in ACS unless you are committed to the cath lab. 2009;95:1701–1706. Morris N, Body R.
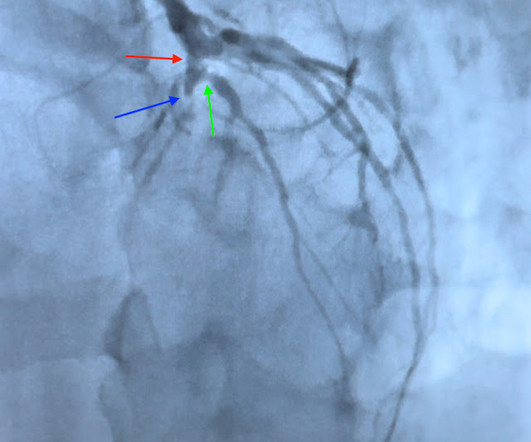
He sent the patient to the ED for further evaluation. A chest x-ray in the ED found bilateral pleural effusions. The scan did not find PE, but showed evidence of coronary plaque: There are areas of dense white in the LAD (red and blue circles) and in the first diagonal (green circle).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content