This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Intermediate-risk patients may be further stratified based on recent stress testing or coronary angiogram findings plus a modified HEART or EmergencyDepartment Assessment of Chest Pain (EDACS) score. The patient has no previous stress testing or coronary angiogram, and he is not low risk by HEART or EDACS scoring.
Case: You are working a busy shift in a rural emergencydepartment (ED) and your excellent Family Medicine trainee presents a case of a 63-year-old woman with chest pain and some intermittent radiation into the inter-scapular region. The patient has no specific risk factors for acute coronary syndrome (ACS) or dissection.
Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Guest Skeptic: Dr. Corey Heitz is an emergency physician in Roanoke, Virginia. He is also the CME editor for Academic Emergency Medicine. Guest Skeptic: Dr. Corey Heitz is an emergency physician in Roanoke, Virginia.
Date: January 16th, 2020 Reference: Troponin Testing and Coronary Syndrome in Geriatric Patients With Nonspecific Complaints: Are We Overtesting? Andrew Huang: Andy is […] The post SGEM#280: This Old Heart of Mine and Troponin Testing first appeared on The Skeptics Guide to Emergency Medicine. Reference: Wang et al.
The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). The patient was rushed to the nearest emergencydepartment (non-PCI facility) for stabilization.
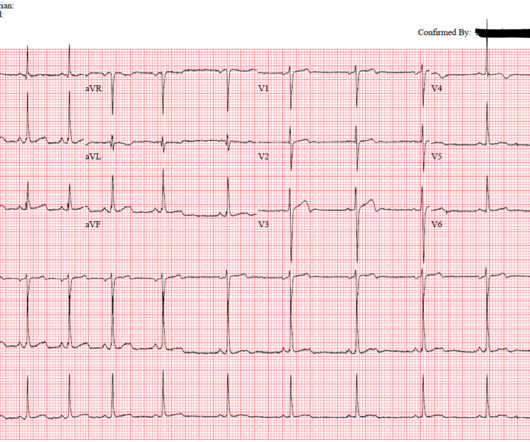
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the EmergencyDepartment via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. What do you think?
She arrives in the emergencydepartment (ED) with decreased level of consciousness and shock. Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients. She has a history of hypertension and non-insulin dependent diabetes mellitus.
Myth 1 Absence of Classic Chest Pain obviates the need for ACS work up The absence of chest pain in no way excludes the diagnosis of ACS. Around 33-50% of the patients with ACS present to the hospital without chest pain. Ann Emerg Med 2002; 40:180–6. Heart 2001; 86:494–8. Gupta M, Tabas JA, Kohn MA. Swap CJ, Nagurney JT.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). ACS and hyperkalemia both have lethal downstream consequences, so it is imperative for the clinician to acclimate to the presentation, or developing, features of each. ECG's are difficult. 2] Costanzo, L.
Guidelines for Reasonable and Appropriate Care in the EmergencyDepartment (GRACE) 2: Low-Risk, Recurrent Abdominal Pain in the EmergencyDepartment. Guidelines for Reasonable and Appropriate Care in the EmergencyDepartment (GRACE) 2: Low-Risk, Recurrent Abdominal Pain in the EmergencyDepartment.
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). They too have dense white masses consistent with coronary atherosclerosis. The blue circle shows the LCx. Murakami MM.
Case 1: Case 2: Case 3: Triage ECGs labeled ‘normal’ There have been a number of small studies suggesting that triage ECGs labeled ‘normal’ are unlikely to have clinical significance, and therefore that emergency physicians should not be interrupted to interpret them, and that such patients can safely wait to be seen.
He arrived in the emergencydepartment hemodynamically stable. ACS would be highly unusual in a young athlete, and given the information on his race bib, one must first suspect that the abnormal ST elevation is due to demand ischemia, not ACS. The next day, and angiogram showed normal coronary arteries.
He presented to the EmergencyDepartment with a blood pressure of 111/66 and a pulse of 117. ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock. Then ACS (STEMI) might be primary; this might be cardiogenic shock. One must clearly rule out these processes before jumping on the ACS diagnosis.
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] It’s judicious, then, to arrange for coronary angiogram.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergencydepartment with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. 2014 AHA/ACC guideline for the management of patients with non-ST elevation acute coronary syndromes.
It is commonly used in EmergencyDepartments, especially in febrile and possibly infectious patients. ACS and Aortic Dissection - For ACS and Dissection, the higher CRP levels, the worse prognosis. It is not used to diagnose ACS/Dissection. Normal levels increase with aging. Utility of CRP 1.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergencydepartment at around 3 AM complaining of chest pain onset around 9 PM the evening prior. Guagliumi, G., Iwaoka, R.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" Chris Mondie of the Newark Beth Israel Emergency Medicine Residency sent case 1 below of a 100% LM occlusion. (ref Widimsky P et al.
This was sent by anonymous The patient is a 55-year-old male who presented to the emergencydepartment after approximately 3 to 4 days of intermittent central boring chest pain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin. It is unknown when this pain recurred and became constant.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. Upon arrival to the emergencydepartment, a senior emergency physician looked at the ECG and said "Nothing too exciting."
, tells us that we physicians do not need to even look at this ECG until the patient is placed in a room because the computer says it is normal: Validity of Computer-interpreted “Normal” and “Otherwise Normal” ECG in EmergencyDepartment Triage Patients I reviewed this article for a different journal and recommended rejection and it was rejected.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergencydepartment with 2 days of heavy substernal chest pain and nausea. Serial ECGs enhance the diagnosis of acute coronary syndrome. Annals of Emergency Medicine , 31 (1), 3–11. link] Fesmire, F.
Notoriously elusive, with a high misdiagnosis rate, thoracic aortic dissection (AD) can mimic many conditions, including acute coronary syndrome (ACS, the most common), gastroesophageal reflux disease (GERD), stroke, and spinal-cord compression. ACS is the most common misdiagnosis and often leads to inappropriate anticoagulation.
A man in his 90s with a history of HTN, CKD, COPD, and OSA presented to the emergencydepartment after being found unresponsive at home. Vital signs were within normal limits on arrival to the EmergencyDepartment. Written by Bobby Nicholson What do you think of this “STEMI”? Blood glucose was not low at 162 mg/dL.
She presented to the emergencydepartment after a couple of days of chest discomfort. Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? The patient is an older woman with known coronary disease and an ICD-Pacemaker implanted because of a history of VT ( V entricular T achycardia ).
Smith: If this is ACS (a big if), t his is just the time when one should NOT use "upstream" dual anti-platelet therapy ("upstream" means in the ED before angiography). History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Anything more on history?
Many conditions outside of acute coronary syndrome (ACS) mimic ST-elevation myocardial infarction (STEMI), but only a handful of cases have reported ST-elevations (STE) in the setting of pancreatic inflammation where underlying ACS was excluded. Click to enlarge.) 2 Proposed hypothesis as described by Hsu et al.,
Written by Kaley El-Arab MD, edits by Pendell Meyers and Stephen Smith A 61-year-old male with hypertension and hyperlipidemia presented to the emergencydepartment for chest tightness radiating to the back of his neck that has been intermittent for the past day or two. What do you think? Stay tuned for upcoming studies showing this.
A 44 year-old male with unknown past medical history came by emergency medical services (EMS) to the emergencydepartment (ED) for an electrical injury and fall from a high voltage electrical pole. 2,3,5 Except for laundry or electrical car outlets (240 V AC), all U.S. household outlets are rated at 120 V AC.
A 35-year-old male presented to the emergencydepartment complaining of chest pain that started 1.5 5 Studies looking at this phenomenon in the emergencydepartment setting for patients presenting with chest pain are lacking. Dr. Young is an emergency physician at Saint Francis Hospital and Medical Center, Hartford, Conn.
A man in his 60s with a history of severe alcohol use disorder and epidural abscess on long-term ciprofloxacin presented to the emergencydepartment after an episode of syncope while standing in line at a grocery store. Moreover, the Queen is only supposed to be used with a high pretest probability of ACS/OMI.
Rather it is due to coronary insufficiency due to a tight left main or 3-vessel disease with inadequate coronary flow. Data collected included demographics, initial rhythm, EKG, emergencydepartment (ED) CT and outcomes. The study population was grouped into those who did and did not have an early CT. Results: Over 8.5
While in the emergencydepartment, he undergoes an additional ECG: 00:49 - Not much change Second ECG with measurements and calculations Magnified view of second ECGs measurements and calculation It is still "negative" for LAD occlusion (less than 23.4) Despite having acute coronary occlusion by cath, his ECGs never met STEMI criteria.
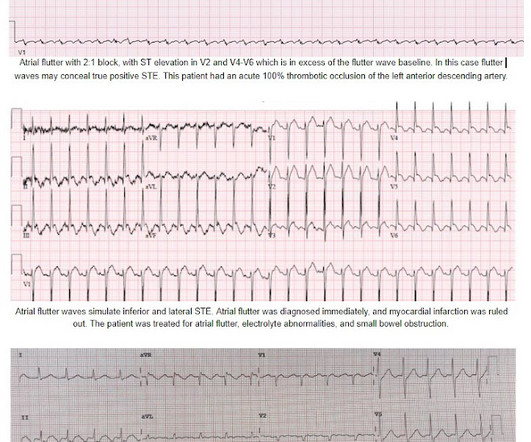
On arrival to the PCI center's EmergencyDepartment, the receiving team recorded an ECG on arrival: Persistent atrial flutter, however this time the QRS occurs on a slightly different portion of the flutter wave. The cardiologist also did not see atrial flutter, and advised giving thrombolytics for perceived "inferior STEMI."
When he showed it to me, I said "Ouch, looks like an acute coronary occlusion. no LBBB or paced rhythm), acute coronary occlusion MI (OMI) is diagnosed in approximately 75% of cases. The Smith-Modified Sgarbossa Criteria Accurately Diagnose Acute Coronary Occlusion in EmergencyDepartment Patients With Ventricular Paced Rhythm.
Because the patient's pain had resolved completely and cardiology had declined immediate intervention, the patient was admitted but continued to board in the emergencydepartment. Approximately 4 hours after arrival, the patient was re-examined by the emergency physician. There is no age cut-off for ACS. 1] Wereski, R.,
He had no symptoms of ACS. The remainder of his EmergencyDepartment stay was uneventful. Here is the clinical informaton on ECG 2: A man in his 50s presented to the EmergencyDepartment with acute chest pain that started within the past few hours. QOH: "OMI High confidence". Physician interpretation: "No STEMI."
A 68-year-old male with a past medical history of hypertension, diabetes mellitus, and coronary artery disease with a drug eluting stent placed 2 months ago presents with dizziness and vomiting that began 3 hours ago. The NIHSS cutoff that predicts outcomes is 4 points higher in AC compared with PC infarctions. Arch Neurol.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergencydepartment with substernal chest pain for 3 hours prior to arrival. The screening physician ordered an EKG and noted his ashen appearance and moderate distress. Triage EKG: What do you think?
And so it is wise to look at the coronary arteries. This ECG certainly looks like myocarditis, and was due to myocarditis, but missing acute coronary occlusion is not acceptable. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease.
She was brought to the EmergencyDepartment and this ECG was recorded while she was still feeling nauseous but denied chest pain, shortness of breath, or other symptoms: What do you think? I wouldn't activate the lab for this EKG alone, but if the patient is clinically compatible with ACS you could call a heart alert.
Here is a video lecture of subtle LAD occlusion: One hour lecture on Subtle ECG Findings of Coronary Occlusion The 3-variable formula comes from this paper: Smith SW et al. consistent with LAD occlusion) This prompted serial ECGs: These dynamic changes confirmed ACS There was a large obtuse marginal 100% occlusion (surprisingly not LAD!
This page summarises the most current recommendations for the management of acute coronary syndromes with persistent ST-segment elevations (i.e I B Patients transferred to PCI centres can bypass the emergencydepartment to undergo primary PCI without delay. STEMI , ST-segment elevation acute myocardial infarction ).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content