This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
David Didlake @DidlakeDW EMS personnel responded to the residence of an 81 y/o Male with syncope. There is increased LV cavity dimensions with an increase in transient ischemic dilation, suggesting Left Main, or 3-vessel coronary artery disease. His spouse had called 911 after she heard a loud “thud” in the adjacent room.
Jesse McLaren on when to consider Spontaneous Coronary Artery Dissection (SCAD), which patients are at risk for reocclusion, and the challenges of diagnosing SCAD in patients who have nonischemic ECGs despite silent occlusion, occlusions perfused by collaterals, or from non-occlusive MI on this ECG Cases.
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. Essentially, we are using the troponin assay to find patients with ACO who may be benefited by coronary interventions or risk factor modification.
EMS arrived and found him in Ventricular Fibrillation (VF). But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. Then assume there is ACS. Smith's ECG Blog ( See My Comment in the March 1, 2023 post) — DSI does not indicate acute coronary occlusion! They started CPR.
Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. The TOMAHAWK Investigators.
According to the EMS narrative, this patient initially refused hospital transport and advised that he would seek evaluation at a later time with his personal physician. According to the EMS narrative, this patient initially refused hospital transport and advised that he would seek evaluation at a later time with his personal physician.
Background: Historically, we have treated acute coronary syndrome with supplemental oxygen regardless of the patient ’ s oxygen saturation. More recent evidence, however, demonstrates that too much oxygen could be harmful ( AVOID Trial ) by causing coronary vasoconstriction and increasing oxidative stress. Low O2 protocol: 3.1%
I interpreted the ECG as VT with two primary etiological possibilities: 1. Abrupt plaque ulceration of Type 1 ACS leading to VT. Ultimately the patient went to Cath and was found to have multi-vessel obstructive coronary disease with an acute LCX culprit vessel, which was stented.
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. It’s judicious, then, to arrange for coronary angiogram. Supply-demand mismatch (non-occlusive coronary disease, or exacerbation of preexisting flow insufficiency) a.
He presented to EMS with extreme pallor, Levine sign, diaphoresis, bilateral arm pain, and an apprehensive sense of doom. It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). In the case of ACS, the ECG can rapidly change from this. ECG's are difficult.
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. Electrocardiographic Differentiation Between Acute Pulmonary Embolism and Acute Coronary Syndromes on the Basis of Negative T Waves - ScienceDirect. looked at consecutive patients with PE, ACS, or neither. What do you think?
We’ll keep it short, while you keep that EM brain sharp. A 68-year-old male with a past medical history of hypertension, diabetes mellitus, and coronary artery disease with a drug eluting stent placed 2 months ago presents with dizziness and vomiting that began 3 hours ago. Lancet Neurol 2009; 8:724-730.
He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic. The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand).
EMS obtained the following vital signs: pulse 50, respiratory rate 16, blood pressure 96/49. It appears EMS obtained two EKGs, but unfortunately these were not saved in the medical record. The EMS crew was only BLS certified, so EKG interpretation is not within their scope of practice. This is not the case.
EMS finds him supine, alert and oriented, and without any gross distress. Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. Crew members note residual pallor and clammy skin. 3] Meyers, H.
RBBB + LAFB in the setting of ACS is very bad. Some patients have baseline RBBB with LAFB, but in patients with likely ACS, these are associated with severe infarction with cardiac arrest, cardiogenic shock or impending shock. Patients with ACS and RBBB/LAFB usually have a left main vs. proximal LAD. Learning Points: 1.
She was known to have a history of poorly controlled COPD, AFib, and multivessel coronary disease. This should prompt immediate investigation into supply-demand mismatching, or ACS. David Didlake, FF/EMT-P, AG-ACNP @DidlakeDW An elder female presented to the ED with worsening shortness of breath. A 12 Lead ECG was captured.
The ECG is just a test: a Bayesian approach to acute coronary occlusion If a patient with a recent femur fracture has sudden onset of pleuritic chest pain, shortness of breath, and hemoptysis, the D-dimer doesn’t matter: the patient’s pre-test likelihood for PE is so high that they need a CT. But does this matter? Amsterdam et al. Lupu et al.
He reported to EMS a medical history of GERD only. V2 – in the final EMS ECG the ST segment was baseline. V3 – in the final EMS ECG the ST segment was still slightly depressed. Cardiology admitted him for observation with plans for next-day coronary angiogram. However, in this context (i.e. 1] Driver, B.
Despite many ECG signs of OMI being missed the door-to-cath time was still fast, because all the healthcare providers were focused on the pathology of acute coronary occlusion and not were distracted by the lack of STEMI criteria. Start using the terms acute coronary occlusion and occlusion MI.
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] It’s judicious, then, to arrange for coronary angiogram.
I was there and said, "No, I think this is all due to severe chronic cardiomyopathy and cardiac arrest due to primary ventricular fibrillation, not due to ACS." _ Why did I say that? For this reason we did not believe this was an acute coronary event and did not activate the cath lab. So we should activate the cath lab, right?
The SGEM bottom line was there is moderate level of evidence that ACS can be excluded in adult patients with recurrent, low-risk chest pain using a single hs-troponin below a validated threshold without further diagnostic testing in patients who have a CCTA within the past two years showing no coronary stenosis.
About 2 hours later the patient arrived at a PCI-capable center and repeat ECG was obtained: The transferring EMS crew noted “runs of VT” during transport. Serial ECGs enhance the diagnosis of acute coronary syndrome. FINAL Point: During transport to the PCI center — the EMS crew noted, "runs of VT". Washam, J. Peacock, W.
Notoriously elusive, with a high misdiagnosis rate, thoracic aortic dissection (AD) can mimic many conditions, including acute coronary syndrome (ACS, the most common), gastroesophageal reflux disease (GERD), stroke, and spinal-cord compression. EMS is called and finds his blood pressure 175/100. Listen to your gut.
We who know ischemic ECGs know that really when T-wave inversion is specific for coronary thrombosis that it indicates reperfusion of the artery, not active occlusion. EMS arrived — and recorded 2 ECGs. 14 minutes later — ECG #2 was recorded by EMS. I personally can hardly wait for that future version! Some patients do this.
Queen of Hearts now thinks that this one looks like posterior OMI, since the STD does appear worst in V3-4: None of this seems to have been understood by the EM doctor or the cardiologist who was consulted. In our opinion it should not be given in ACS unless you are committed to the cath lab. He was diagnosed as NSTEMI.
With EMS, patient had a GCS of 3 and was saturating 60% on room air. He improved to 100% with the addition of non-rebreather, however remained altered and was intubated by EMS with ketamine and succinylcholine. Preliminary findings documented in the cath lab were “Anterior STEMI and no significant coronary artery disease.” (!!!)
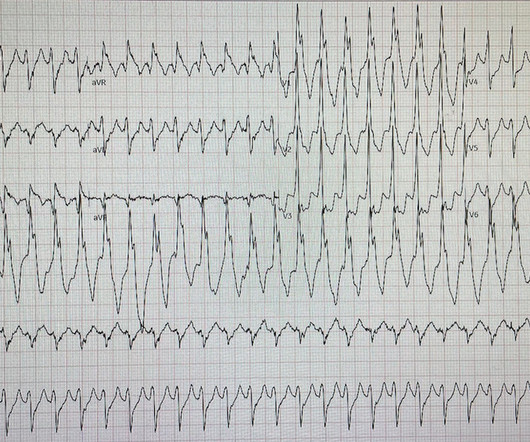
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chest pain. Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. Smith adds to our knowledge of this syndrome.
Click here for Direct Download of the Podcast Paper: Aykan AC et al. PMID: 23102885 Aykan AC et al. appeared first on REBEL EM - Emergency Medicine Blog. Because the lungs receive 100% of cardiac output, it has been hypothesized that a lower dose of thrombolytic therapy may still be effective with a better safety profile [3][4].
All patients with NSTE-ACS ( NSTEMI or unstable angina) are treated similarly with respect to anti-ischemic and anti-thrombotic drugs. Management must, however, be individualized with respect to the delay to coronary angiography (PCI). TIMI Risk Scores for NSTE-ACS (NSTEMI, UA) and STE-ACS ( STEMI ) can be calculated below.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. One need not have obstructive coronary disease to have occlusive thrombus!
He reported a history of ischemic cardiomyopathy with coronary stent placement approximately 10 years prior, but could not recall the specific artery involved. Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion. Attached is the first ECG.
A 44 year-old male with unknown past medical history came by emergency medical services (EMS) to the emergency department (ED) for an electrical injury and fall from a high voltage electrical pole. Per EMS, the patient was found at the bottom of a high voltage line with diffuse burns and amputation of his left forearm. Emerg Med Pract.
She took an oxycodone and called EMS. The patient was thought to have low likelihood of ACS, and cardiology recommended repeat troponin, urine drug testing, and echocardiogram. At that point, cardiology elected to treat for ACS. Another option would be to use Optical Coherence Tomography for Coronary Imaging ).
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chest pain, weakness and nausea. En route, EMS administered aspirin 325mg by mouth, but withheld nitroglycerin due to initial hypotension. Answer below in the still shot.
If this is ACS with Aslanger's pattern , the ST depression vector of subendocardial ischemia (due to simultaneous 3 vessel or left main ACS) is directed toward lead II (inferior and lateral). Thus, this apparently is Aslanger's Pattern (inferior OMI with single lead STE in lead III, with simultaneous subendocardial ischemia).
The EM provider asked if the cardiologist thought it was a "STEMI." Second, the increased demand created by extreme tachycardia may exceed the ability of the coronary arteries to supply sufficient blood (due to preexisting three vessel or left main disease, with or without ACS).
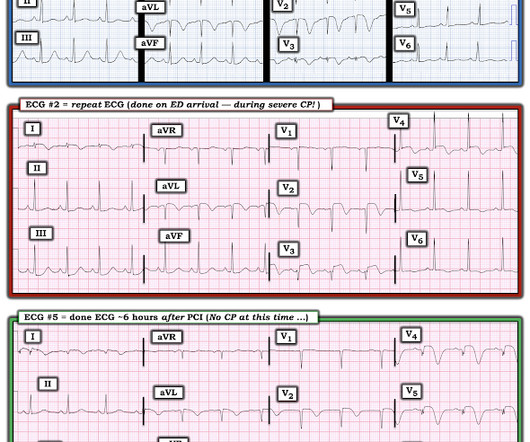
This is acute ACS, but it almost always seen in a pain free state. Smith — in the setting of a patient with new chest pain — the initial ECG in today's case ( = ECG #1 — obtained by the EMS team prior to ED arrival ) — is diagnostic of ACS ( A cute C oronary S yndrome ) until proven otherwise.
Acute coronary occlusion is the most common and most treatable cause of this pattern, but it is not the only cause. Takotsubo, spasm, low flow with a preexisting stable coronary lesion, etc. The myocytes do not know why they are dying, they can only report their death and hope you can see it and figure it out.
Today’s pain lasted around 20 mins, but was severe enough that the patient called EMS. Pain largely resolved prior to EMS arrival but completely subsided after prehospital NTG and aspirin. There is no age cut-off for ACS. At the time of arrival to the ED, the patient reported 1/10 chest pain with normal vital signs.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin.
Submitted and written by Quinton Nannet, MD, peer reviewed by Meyers, Grauer, Smith A woman in her 70s recently diagnosed with COVID was brought in by EMS after she experienced acute onset sharp midsternal chest pain without radiation or dyspnea. cm distal to the non-coronary cusp of the aortic valve."
It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chest pain. This is step 4 : relying on the first troponin level to rule out acute coronary occlusion. 4] CT revealed no dissection but extensive coronary atherosclerosis.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content