This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He denied any specific prodrome of gross palpitations, however did endorse feeling quite dizzy just before the event. Given no clinical prelude of anginal (or equivalent) descriptors, prior to the acute event, risk stratification of the ECG and Troponin was pursued via Echo and nuclear Myocardial Perfusion Imaging (MPI).
Compensatory enlargement was defined as being present when the total coronary arterial cross-sectional area at the stenotic site was greater than that at the proximal nonstenotic site. Furthermore, if this occurs at all, it is a rare event. Unfortunately, vascular remodeling is variable and inconsistent.
Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? He has no history of coronary artery disease. If we thought about ACS, we brought them in. AEM June 2022.
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. Essentially, we are using the troponin assay to find patients with ACO who may be benefited by coronary interventions or risk factor modification.
Myth 1 Absence of Classic Chest Pain obviates the need for ACS work up The absence of chest pain in no way excludes the diagnosis of ACS. Around 33-50% of the patients with ACS present to the hospital without chest pain. Close to 20% of patients diagnosed with acute MI present with symptoms other than chest pain.
For the same reason, you should not delay coronary angiography because pain resolves with morphine. Smith : As Willy states, ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). But pain is a critical signal for urgency in the context of acute coronary syndrome. Worrall, C.,
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). They too have dense white masses consistent with coronary atherosclerosis. The blue circle shows the LCx.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. This is not the case.
I was there and said, "No, I think this is all due to severe chronic cardiomyopathy and cardiac arrest due to primary ventricular fibrillation, not due to ACS." _ Why did I say that? For this reason we did not believe this was an acute coronaryevent and did not activate the cath lab. So we should activate the cath lab, right?
More past history: hypertension, tobacco use, coronary artery disease with two vessel PCI to the right coronary artery and circumflex artery several years prior. This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. It is unknown when this pain recurred and became constant.
We who know ischemic ECGs know that really when T-wave inversion is specific for coronary thrombosis that it indicates reperfusion of the artery, not active occlusion. that is, show a pattern of labile ST-T wave changes not due to an acute coronaryevent. I personally can hardly wait for that future version!
There were zero patients in this study with a "normal" ECG who had any kind of ACS! Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. So this study is actually worthless.
A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD Although a lesion is not visible anatomically on this CT scan, coronary catheter angiography could be considered based on Cardiology evaluation." A repeat troponin returned at 0.45 CAD-RADS category 1. --No
The biphasic T wave is consistent with recent reperfusion of an occluded coronary artery supplying the inferior region. Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA.
In our opinion it should not be given in ACS unless you are committed to the cath lab. Learning Point: Any NSTEMI patient with active ongoing ACS symptoms refractory to medical management is supposed to go to the cath lab within 2 hours if available, per all guidelines in world, regardless of ECG findings. 2009;95:1701–1706.
Thus, these troponins are very concerning for ACS, and subsequent ones will probably be diagnostic of acute MI. We know that even high-sensitivity troponin may not exceed the "normal" range for a period of hours in certain patients with acute coronary occlusion. The troponin is trapped in the myocardium that is not being perfused.
Click here for Direct Download of the Podcast Paper: Aykan AC et al. PMID: 23102885 Aykan AC et al. Because the lungs receive 100% of cardiac output, it has been hypothesized that a lower dose of thrombolytic therapy may still be effective with a better safety profile [3][4]. Clin Exp Emerg Med 2023. in the paper but 2.7%
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Association of intravenous morphine use and outcomes in acute coronary syndromes: Results from the CRUSADE Quality Improvement Initiative.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. Takotsubo is a sudden event, not one with crescendo angina. Such cases are classified as MINOCA (Myocardial Infarction with Non-Obstructed Coronary Arteries).
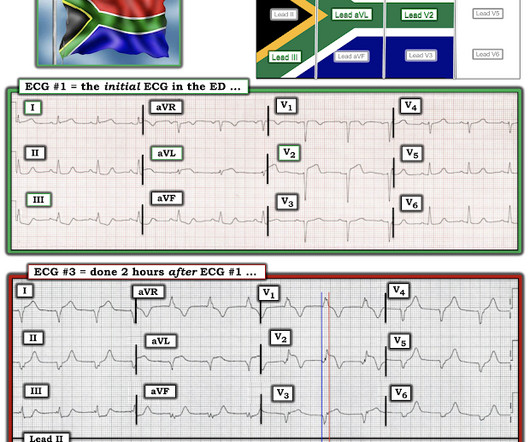
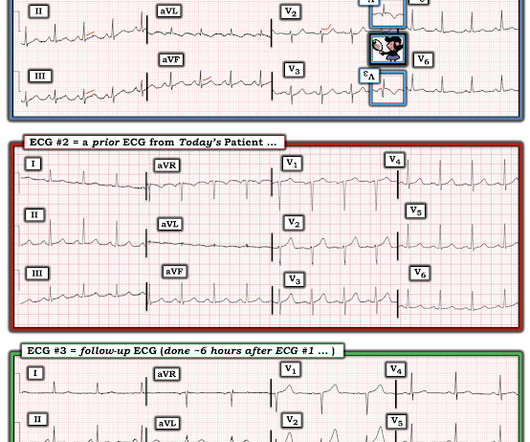
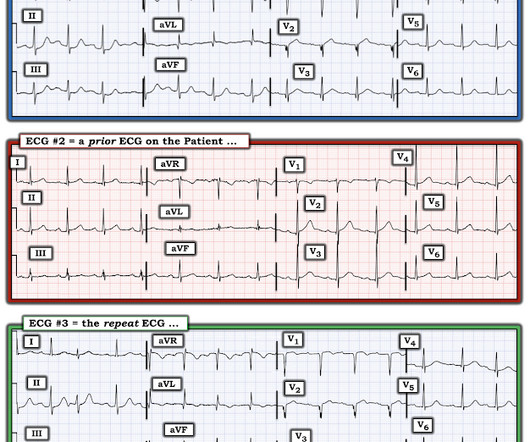
No wall motion abnormality This shows that significant ACS can have ZERO WMA!! A comparison of electrocardiographic changes during reperfusion of acute myocardial infarction by thrombolysis or percutaneous transluminal coronary angioplasty. And dynamic ST-T wave changes between ECG #1 and ECG #2 confirm an acute event in progress.
Subsequent events: Later, before being taken to her room, the 2nd troponin returned at 1.01 Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. What is Spontaneous Coronary Artery Dissection (SCAD)? She felt more comfortable being admitted.
Here is the post shock ECG: Cardiology was called stat for ischemic VT, query SCAD vs thrombotic occlusion vs coronary vasospasm. Cath lab was activated: There was no coronary artery disease, but there was spontaneous coronary artery dissection (SCAD) of the distal LAD, which was narrowed by 95%, and treated medically.
He reported a history of ischemic cardiomyopathy with coronary stent placement approximately 10 years prior, but could not recall the specific artery involved. Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion. Attached is the first ECG.
But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Dialysis patients have a high rate of ACS without chest pain and high rate of delayed diagnosis and delayed reperfusion 2.
But there are also hyperacute T waves (HATW) in V4-5, which exclude early repolarization and pericarditis, leaving only LAD occlusion for this patient presenting with classic symptoms of ACS. Not whether there was or was not Acute Coronary Occlusion. Not whether the ST segments met STEMI millimeter criteria. _
I did not think it was due to ACS, but we ordered an ED ECG immediately: What do you think? But in this case the clinical scenario is not right for acute ACS with OMI, and there is very high voltage, and the patient is very young, (though beware of young patients , even 29 year olds!! I was not worried for a coronary etiology.
The AHA/ACC guidelines recommend emergent cardiac catheterization for patients with concern for ACS and refractory chest pain despite maximum medical therapy defined as aspirin + clopidogrel/ticagrelor + heparin/enoxaparin. link] He was admitted to the cardiology unit for serial troponin measurements and concern for possible ACS.
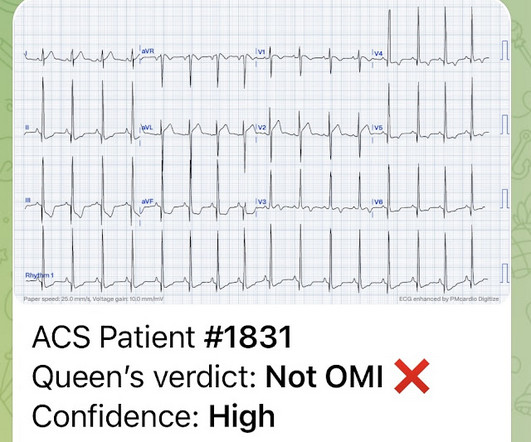
Moreover, the Queen is only supposed to be used with a high pretest probability of ACS/OMI. Instead — it commonly reflects ischemia from severe underlying coronary disease. We just finished training version 2 with some cases of hypokalemia, so that is in the future. Magnesium later resulted at 0.8 mg/dL, and ionized calcium was 0.73
No obvious adverse events were attributed to the thrombolytics. Second, the increased demand created by extreme tachycardia may exceed the ability of the coronary arteries to supply sufficient blood (due to preexisting three vessel or left main disease, with or without ACS). There was again no intracranial hemorrhage.
The patient was thought to have low likelihood of ACS, and cardiology recommended repeat troponin, urine drug testing, and echocardiogram. At that point, cardiology elected to treat for ACS. Another option would be to use Optical Coherence Tomography for Coronary Imaging ). Initial hscTnI was 10 ng/L (ref. <14).
I showed this to some of my colleagues and they were not able to confidently say that this is an acute coronary occlusion. Guidelines say that if a patient has ACS but refractory pain, the patient should go emergently to the cath lab. Back to the case. Initial troponin I returned elevated at 84 ng/L (ref value <34 ng/L).
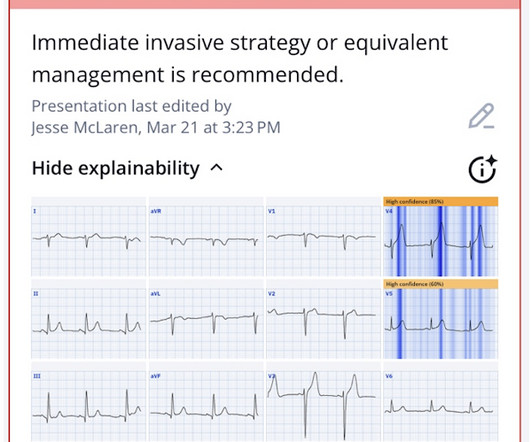
ST depression maximal in V1-V4, in the context of ACS symptoms and unexplained by QRS abnormality or tachydysrhythmia, should be considered posterior OMI until proven otherwise. Today's patient is high-risk ( ie, in a high "prevalence" group for having an acute coronaryevent ).
It is easy to say this in retrospect, especially not being the one in charge of this overcrowded waiting room full of unseen patients, but an elderly patient with known CAD and ongoing ACS-sounding chest pain despite medical management with positive troponin is already an indication for emergent cath, regardless of the ECG!
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion).
The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Author continued : STE in aVR is often due to left main coronary artery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58).
Acute coronary occlusion is the most common and most treatable cause of this pattern, but it is not the only cause. Takotsubo, spasm, low flow with a preexisting stable coronary lesion, etc. The myocytes do not know why they are dying, they can only report their death and hope you can see it and figure it out.
The patient would not have been diagnosed with acute coronary syndrome and would not have had an angiogram, would have been discharged (or perhaps had a stress test, which would be negative), and would be at great risk of another event, possibly resulting in death or heart failure. Imagine if you had only recorded the 2nd ECG.
Recall that, in the setting of ACS symptoms, ST depression that are maximal in leads V1-V4 (as opposed to V5 and V6) not attributable to an abnormal QRS complex is specific for OMI. The most recent event had occurred just before being triaged. This pattern is recognizable by the ST depressions maximal in lead V4.
Wellens pattern is a term which refers to coronary reperfusion morphology in the anterior leads) The best answer is because the entire gestalt of the ECG shows acute right heart strain instead, and just does not look like Wellens after you've seen Wellens hundreds of times. looked at consecutive patients with PE, ACS, or neither.
Corroborating this is the subtle ST depression in V2-V3 which is inappropriate for the normal QRS complex, and in the context of ACS, we have shown this is quite specific for posterior OMI. In the context of ACS, ST depression maximal in V1-V4 (rather than V5-V6) not due to a QRS abnormality is specific for posterior OMI.
Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion. As he documented, “This patient is experiencing chest pain consistent with an acute coronary syndrome. Start using the terms acute coronary occlusion and occlusion MI. That’s exactly what happened in this case.
Considering hyperacute T-waves have been accepted as STEMI equivalents, it is possible that pseudonormalization could gain more recognition as an indicator of ACS. Sequence of events in angina at rest: Primary reduction in coronary flow. Normalization of abnormal T waves in ischemia. Arch Intern Med. 1976 Apr;136(4):391-5.
For coronary anatomy, see here: [link] This is the post intervention ECG: All ST Elevation is gone (more proof that it was all a result of ischemia) Formal Echo: Normal estimated left ventricular ejection fraction - 55%. K EY P oints : This patient has known coronary disease. It was stented.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content