This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Madden, Paramedic. It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). An interesting comment provided by Paramedic Madden is that a few team members initially interpreted the T wave presentation as hyperkalemia, as opposed to occlusive hyperacuity.
The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation. Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients. EMS arrives and finds the patient in monomorphic ventricular tachycardic (VT) cardiac arrest.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review provided by Dr. Steve Smith @SmithECGblog I was conducting QA/QI on two very recent cases and was struck by the uniqueness of both. It’s important to stress the presence of a normal QRS (i.e., This ECG immediately struck me as an LAD occlusion.
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (ret) @DidlakeDW Expert commentary and peer review by Dr. Steve Smith [link] @smithECGBlog A 57 y/o Female with PMHx HTN, HLD, DM, and current use of tobacco products, presented to the ED with chest discomfort. It’s judicious, then, to arrange for coronary angiogram.
She was known to have a history of poorly controlled COPD, AFib, and multivessel coronary disease. This should prompt immediate investigation into supply-demand mismatching, or ACS. Pharmacology Review Digoxin is probably one of those medications vaguely recalled from paramedic school. A 12 Lead ECG was captured.
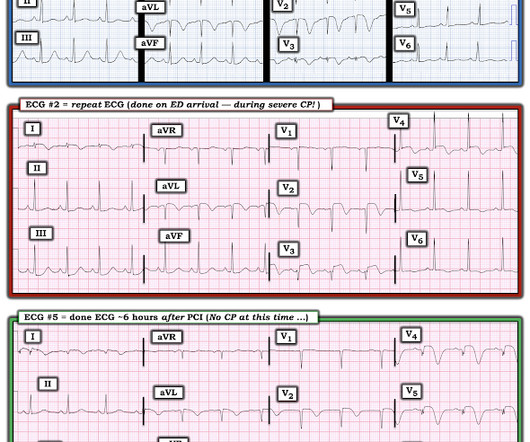
Below is the first ECG recorded by paramedics after 2 hours of chest pain, interpreted by the machine as “possible inferior ischemia”. In isolation this ECG does not show OMI, but following the paramedic ECGs this indicates spontaneous LAD reperfusion. It’s unclear if the paramedic ECGs were seen or missed in the ED.
Paramedics provided another 3 sprays of nitro, and 6mg of morphine, which reduced but did not resolve the pain. Similarly, if a patient with known CAD presents with refractory ischemic chest pain, the ECG barely matters: the pre-test likelihood of acute coronary occlusion is so high that they need an emergent angiogram. Alencar et al.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. One need not have obstructive coronary disease to have occlusive thrombus!
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Expert commentary provided by Dr. Ken Grauer CASE 1 An 82 y/o Male called 911 for sudden onset dizziness while at rest. Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Look at the aortic outflow tract.
This is acute ACS, but it almost always seen in a pain free state. Smith — in the setting of a patient with new chest pain — the initial ECG in today's case ( = ECG #1 — obtained by the EMS team prior to ED arrival ) — is diagnostic of ACS ( A cute C oronary S yndrome ) until proven otherwise.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review provided by Dr. Steve Smith [link] @SmithECGblog A 72 y/o Male experiences a syncopal episode while seated. Evaluation of T-wave morphology in patients with left bundle branch block and suspected acute coronary syndrome. 3] Meyers, H.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review by Dr. Stephen Smith @smithECGblog I was reviewing ECG’s in our LifeNet database and happened upon this one without any knowledge of clinical circumstances. Cardiology admitted him for observation with plans for next-day coronary angiogram.
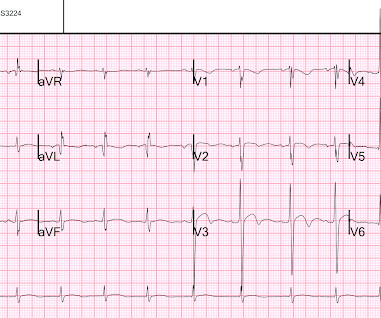
Here’s the paramedic ECG (digitized by PMcardio). According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists. HR 40, BP 135/70, RR16, O2 100%. What do you think?
This was shown to me by a very astute Hennepin paramedic. Although this comes from a Hennepin paramedic, the patient was not brought to Hennepin County Medical Center. It is important for cardiologists to realize that a paramedic may see something they do not. of this post. This is my reponse. This is not tribalism.
She was found by paramedics with an oxygen saturation of 64%, but could not tolerate BiPAP during transport due to claustrophobia. The scan showed a bicuspid aortic valve with severe stenosis and coronary artery disease. She awoke in the morning with sharp chest pain which worsened throughout the morning.
Pretty impressive for someone who has not yet attended med school, or even been a nurse or paramedic yet. html ) Despite an undetectable troponin and three normal EKGs, the nature of the patients symptoms and his positive cardiac history warranted concern for ACS. This interpretation was confirmed by the overreading physician.
A comparison of electrocardiographic changes during reperfusion of acute myocardial infarction by thrombolysis or percutaneous transluminal coronary angioplasty. Here is a case that shows how Wellens' pattern evolves from a subtle OMI (Case 3): Paramedics make a great call A middle-aged male called 911 for chest pain. Penn, Hein J.J.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content