This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
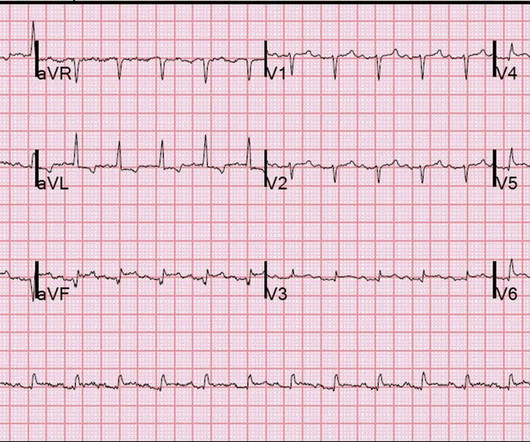
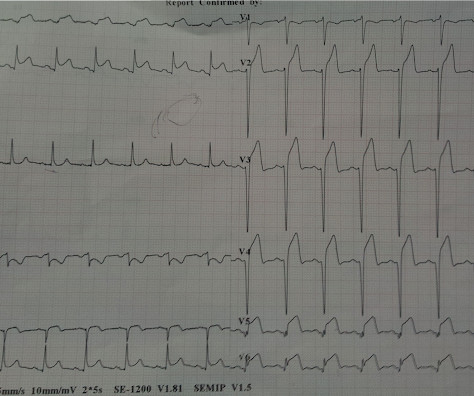
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. Compensatory enlargement was defined as being present when the total coronary arterial cross-sectional area at the stenotic site was greater than that at the proximal nonstenotic site. He was started on nitro gtt.
Jesse McLaren on when to consider Spontaneous Coronary Artery Dissection (SCAD), which patients are at risk for reocclusion, and the challenges of diagnosing SCAD in patients who have nonischemic ECGs despite silent occlusion, occlusions perfused by collaterals, or from non-occlusive MI on this ECG Cases.
But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. Then assume there is ACS. Cardiac arrest #3: ST depression, Is it STEMI? Smith's ECG Blog ( See My Comment in the March 1, 2023 post) — DSI does not indicate acute coronary occlusion! And what do you want to do?
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Similarly, if a patient with known CAD presents with refractory ischemic chest pain, the ECG barely matters: the pre-test likelihood of acute coronary occlusion is so high that they need an emergent angiogram.
Although the attending crews did not consider the ECG pathognomonic for occlusive thrombosis, they nonetheless considered the patient high-risk for ACS and implored him to reconsider. A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. The pathology is now painfully evident.
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. Do NOT give it unless you are committed to the cath lab!! Cath attending is aware. It is a mass delusion.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." For the same reason, you should not delay coronary angiography because pain resolves with morphine. The case continues.
Background: Historically, we have treated acute coronary syndrome with supplemental oxygen regardless of the patient ’ s oxygen saturation. More recent evidence, however, demonstrates that too much oxygen could be harmful ( AVOID Trial ) by causing coronary vasoconstriction and increasing oxidative stress. Low O2 protocol: 3.1%
He was rushed by residents into our critical care room with a diagnosis of STEMI, and they handed me this ECG: There is sinus tachycardia with ST elevation in II, III, and aVF, as well as V4-V6. At first glance, it seems the patient is having a STEMI. ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock.
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). They too have dense white masses consistent with coronary atherosclerosis. The blue circle shows the LCx.
Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients. There is evidence that taking those patients with ROSC and EKG showing STEMI directly for angiography +/- angioplasty is associated with positive patient-oriented outcomes.
These have all been small studies, studying very few patients with ACS, and often used final cardiology interpretation rather than patient outcome. Smith : This study had such low risk patients that not a single patient was ultimately diagnosed with ACS. It is well known that NOMI usually has a normal ECG or nonspecific ECG.
This is as clear a STEMI as you can get. Now, it is true that shortly after a non-ACS cardiac arrest, there can be transient diffuse ST depression, but not ST elevation in a coronary distribution, and there should not be a wall motion abnormality. This could not have been known without the angiogram.
There were zero patients in this study with a "normal" ECG who had any kind of ACS! Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. So this study is actually worthless. Deutch et al.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. This case is an example of the steps we can all take in daily practice as the paradigm shifts from STEMI to OMI.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). ACS and hyperkalemia both have lethal downstream consequences, so it is imperative for the clinician to acclimate to the presentation, or developing, features of each. ECG's are difficult. 2] Costanzo, L.
Many conditions outside of acute coronary syndrome (ACS) mimic ST-elevation myocardial infarction (STEMI), but only a handful of cases have reported ST-elevations (STE) in the setting of pancreatic inflammation where underlying ACS was excluded. 2 Proposed hypothesis as described by Hsu et al., Click to enlarge.)
I sent this ECG to the Queen of Hearts (PMcardio OMI), and here is the verdict: You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form Then I learned that a Code STEMI was activated for concern of anterior "STEMI" in V1-V2. High sensitivity troponin I was 23 ng/L.
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." Electrocardiographic Differentiation Between Acute Pulmonary Embolism and Acute Coronary Syndromes on the Basis of Negative T Waves - ScienceDirect. In fact, Kosuge et al. Accessed May 28, 2024.
ACS would be highly unusual in a young athlete, and given the information on his race bib, one must first suspect that the abnormal ST elevation is due to demand ischemia, not ACS. The next day, and angiogram showed normal coronary arteries. An echocardiogram confirmed aortic stenosis with a large pressure gradient.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery? Widimsky P et al.
More past history: hypertension, tobacco use, coronary artery disease with two vessel PCI to the right coronary artery and circumflex artery several years prior. He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. So it can miss some OMI.
BP 142/100 HR 90 RR 16 (BBS CTA) SpO2 99 (RA) Dstick 110 My colleagues noted the ST-depression in the respective leads, as well, and STEMI activated to the nearest PCI center. 1] Here is the admitting ED ECG after cancellation of Code STEMI. Cardiology admitted him for observation with plans for next-day coronary angiogram.
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] STEMI was activated and the patient went to Cath on arrival.
This ECG was read as “No STEMI” with no prior available for comparison. It is true this ECG does not meet STEMI criteria (there is 1.0 The patient has also developed sinus bradycardia, which may result from right coronary artery ischemia to the SA node. Instead we discussed 5 minute delays for the STEMI(+) OMI patients.
Emergent coronary angiography is not recommended over a delayed or selective strategy in patients with ROSC after cardiac arrest in the absence of ST-segment elevation, shock, electrical instability, signs of significant myocardial damage, and ongoing ischemia (Level 3: no benefit). COR 2a, LOE B-R. COR 1, LOE B-NR. COR 2a, LOE B-NR.
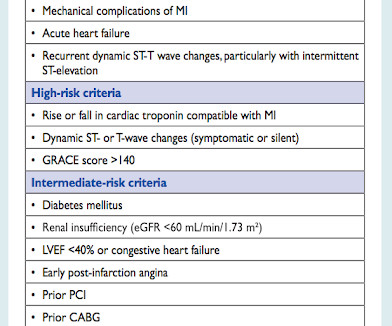
All patients with NSTE-ACS ( NSTEMI or unstable angina) are treated similarly with respect to anti-ischemic and anti-thrombotic drugs. Management must, however, be individualized with respect to the delay to coronary angiography (PCI). TIMI Risk Scores for NSTE-ACS (NSTEMI, UA) and STE-ACS ( STEMI ) can be calculated below.
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). With EMS, patient had a GCS of 3 and was saturating 60% on room air. Version 2 = 0.0272.
Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Day 12 ECG: FINAL DIAGNOSIS: "NSTEMI" Despite the fact that his day 4 ECG easily meets STEMI criteria, the patient is diagnosed as NSTEMI. No TIMI flow was listed in the report. Am Heart J.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. This is not the case.
The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Serial ECGs enhance the diagnosis of acute coronary syndrome. Is there STEMI? Association of intravenous morphine use and outcomes in acute coronary syndromes: Results from the Crusade Quality Improvement Initiative.
You can see how V1, V2, aVR, and V4R would have ST elevation in either a right ventricular STEMI or with a septal STEMI, and how lateral leads, and even posterior leads, would have reciprocal ST depression. of patients with anterior STEMI, ST elevation of greater than or equal to 3.0 STE in V4R is confirmatory evidence.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. This is not unusual. Take home 1.
This patient could have very easily been overlooked, both because the ECG was STEMI negative and because the Q waves were attributed to an “old infarct”. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion. OMI or STEMI? As cardiology documented, “possible STEMI.
He had some cardiac risk factors including hypertension, on meds, but no previous coronary disease. He had an immediate ED ECG: There is artifact, but the findings appear to be largely gone now The diagnosis is acute MI, but not STEMI. His pain was intermittent and he was vague about when it was present and when it was resolved.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. His response: “subendocardial ischemia. Anything more on history? POCUS will be helpful.”
A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD Although a lesion is not visible anatomically on this CT scan, coronary catheter angiography could be considered based on Cardiology evaluation." Transient STEMI is at high risk of re-occlusion.
Furthermore, the term "STEMI equivalent" has no reliable or definable meaning except between two practitioners who both agree on the list of entities that they believe are STEMI equivalents and can agree on how to identify it. Obvious inferoposterior STEMI. J ACC 61(4):e78-140; page e83.
Does this patient have ACS? He did not have ACS. Ventricular fibrillation is not only caused by acute coronary syndrome. We found that 38% of out of hospital ventricular fibrillation was due to STEMI. The remainder were due to other etiologies, (including NonSTEMI ACS). The patient was cardioverted.
The "criteria" for posterior STEMI are 0.5 Is it STEMI or NonSTEMI? We could not rule out acute epicardial coronary (large artery) occlusion. It was opened and stented with a door to balloon time of about 120 minutes (this is long for STEMI, but very short for a high risk Non STEMI). The troponin I returned at 4.1
Comment Notice that I did not even put ACS on my differential? These ECGs, in my experience, are not seen in ACS. However, there are morphologies of Takotsubo that cannot be distinguished from STEMI. Takotsubo This looks like and infero-posterior STEMI, but the QT is bizarrely long. The angiogram was negative."
Here is the post shock ECG: Cardiology was called stat for ischemic VT, query SCAD vs thrombotic occlusion vs coronary vasospasm. Cath lab was activated: There was no coronary artery disease, but there was spontaneous coronary artery dissection (SCAD) of the distal LAD, which was narrowed by 95%, and treated medically.
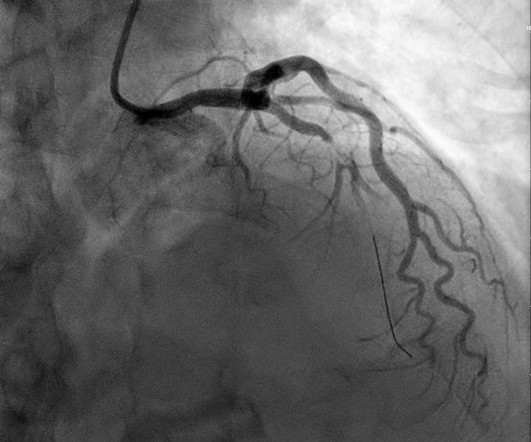
The biphasic T wave is consistent with recent reperfusion of an occluded coronary artery supplying the inferior region. Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content