This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
They started CPR. The patient was brought to the ED and had this ECG recorded: What do you think? Then assume there is ACS. This patient was witnessed by bystanders to collapse. EMS arrived and found him in Ventricular Fibrillation (VF). He was defibrillated into VT. After 1 mg of epinephrine they achieved ROSC.
He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP). The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation.
There was no bystander CPR. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines.
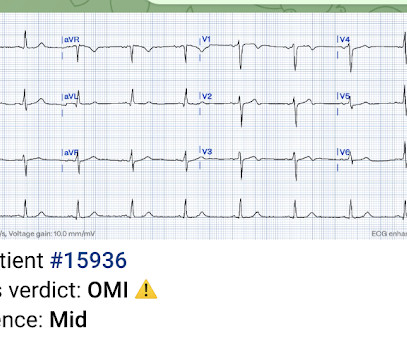
This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. 3-vessel disease can make resuscitation very difficult, since CPR does not perfuse diseased vessels as well as one would like. In aVF it is "coved" (upwardly convex). There is ischemic ST depression in V4-V6. Figure-1: The initial ECG in today's case.
This post will focus on the key parts of the guideline that affect ED evaluation and management. For patients with OHCA, use of steroids during CPR is of uncertain benefit. Editorial Comment: ECPR may be considered in patients refractory to standard ACS in the right situation. COR 2b, LOE B-R. COR 2b, LOE C-LD. COR 2a, LOE B-R.
This is supplied via alternating current (AC), increasing the risk of titanic contraction of skeletal muscle, leading to kids holding on to the electrical power source. Prolonged CPR should be considered as outcomes are generally good, even if asystole is the presenting rhythm. AC and DC shocks may result in different injury patterns.
It was witnessed, and CPR was performed by trained individuals. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. Here is an article I wrote: Updates on the ECG in ACS. at the time of the ECG.
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. CPR was initiated immediately. It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation.
This single-centre academic urban institution in the United States (US) undertook a 10-year retrospective observational study of paediatric intubation and bougie use in their emergency department (ED). During a 6-month period, paediatric patients (< 18 years old) who underwent tracheal intubation in their ED were included in the study.
Case A 42-year-old lady presented to the ED with complaints of intermittent episodes of chest pain associated with shortness of breath for the last 2 days. CPR was initiated and she subsequently entered into V-Fib storm. If this patient was discharged from the ED she very likely would have died. Thanks, Sam! Normal ECG.”
Medics found her apneic and pulseless, began CPR, and she was found to be in asystole. She was hypotensive in the ED and her bedside echo showed a normal RV and LV. Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR.
A 67-year-old man presents to the emergency department (ED) in cardiac arrest. On ED presentation, he is unresponsive and the monitor shows ventricular fibrillation. Emmerson AC, Whitbread M, Fothergill RT. He was found by bystanders after he collapsed and 911 was called. Canadian Journal of Emergency Medicine. 20(S1):S67.
Smith and Meyers answer: First , LM occlusion is uncommon in the ED because most of these die before they can get a 12-lead recorded. Only 28% of patients had ACS of any vessel, and, of those patients, the LM was the culprit in just 49% (14% of all cases).(56) Of those who do get to the ED, many present with clear STE.(65,
Optimally, bystander CPR, including the administration of rescue breaths, should be initiated prior to arrival of emergency medical services. ED treatment should focus on airway, breathing, and circulation with consideration for cervical spine protection depending on the circumstances surrounding the event. South Med J. Acad Emerg Med.
The patient arrived in the ED and had this ECG recorded: Interpretation? It is highly associated with proximal LAD occlusion or severe left main ACS and with bad outcomes. But the clinical history is not compatible with STEMI, so one must be very cautious about the ECG interpretation. The medics activated the cath lab.
About an hour later, he was then found on the floor in cardiac arrest in the ED. He underwent CPR and then was shocked out of VF. ST depression maximal in V1-V4, in the context of ACS symptoms and unexplained by QRS abnormality or tachydysrhythmia, should be considered posterior OMI until proven otherwise.
PMID: 30060961 Koller AC, et al. I would rather use a PCAC score to decide on transfer than arrest characteristic (time of CPR, initial rhythm, etc) because we know that all of that data is prone to bias as well. Epub 2016 Jun 28. PMID: 27368428 Elmer J, et al. Ann Emerg Med. Epub 2018 Jul 4. Resuscitation.
This is a 30-something healthy patient presented with COVID pneumonia who presented to the ED. He underwent CPR, and regained a pulse after epinephrine, with an organized narrow complex rhythm at 140, but still with severe shock. of Cardiology AC, Others. He was moderately hypoxic. He was intubated and then went pulseless.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content