This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
They started CPR. Then assume there is ACS. Cardiac arrest #3: ST depression, Is it STEMI? This patient was witnessed by bystanders to collapse. EMS arrived and found him in Ventricular Fibrillation (VF). He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. sodium bicarbonate.
The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation. Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients. EMS arrives and finds the patient in monomorphic ventricular tachycardic (VT) cardiac arrest.
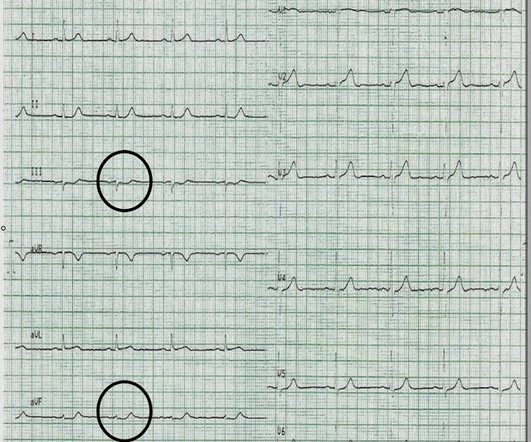
He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. Sensitivity was 87% for OMI in our validation study (it was 34% for STEMI criteria). So it can miss some OMI.
For patients with OHCA, use of steroids during CPR is of uncertain benefit. Extracorporeal CPR Use of ECPR for patients with cardiac arrest refractory to standard ACLS is reasonable in select patients when provided within an appropriately trained and equipped system of care. COR 2b, LOE B-R. COR 2b, LOE C-LD. COR 2a, LOE B-R.
It was witnessed, and CPR was performed by trained individuals. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. Here is an article I wrote: Updates on the ECG in ACS. The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI.
Medics found her apneic and pulseless, began CPR, and she was found to be in asystole. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Kurkciyan et al.
But if they do present: The very common presentation of diffuse STD with reciprocal STE in aVR is NOT left main occlusion , though it might be due to sub total LM ACS, but is much more often due to non-ACS conditions, especially demand ischemia. All are, however, clearly massive STEMI.
It may be difficult to read STEMI in the setting of RBBB. There is, however, a long QT also, with abnormal T-waves, but this is not STEMI. This ECG was recorded prehospital, and the computer read STEMI, so the medics activated the cath lab: What do you think? The ECG is consistent with high lateral STEMI. Called 911.
CPR was initiated immediately. If this is ACS with Aslanger's pattern , the ST depression vector of subendocardial ischemia (due to simultaneous 3 vessel or left main ACS) is directed toward lead II (inferior and lateral). It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation.
He underwent immediate CPR, was found to be in ventricular fibrillation, and was successfully resuscitated. Therefore, even with a normal or non-diagnostic ECG, a 50 year old male patient should undergo serial ECGs and troponins and be admitted to a monitored bed until MI or ACS can be ruled out. See explanation below.
Data that do not establish neurological risk stratification in the first 6 hours after CA include the patient’s age, duration of CPR, seizure activity, serum lactate level or pH, Glasgow motor subscore in patients who received NMB or sedation, pupillary function in patients who received atropine, and optic nerve sheath diameter (95.3%, 20/21).
He underwent CPR and then was shocked out of VF. ST depression maximal in V1-V4, in the context of ACS symptoms and unexplained by QRS abnormality or tachydysrhythmia, should be considered posterior OMI until proven otherwise. His initial troponin T was 15 ng/L (only two hours since pain onset).
He underwent CPR, and regained a pulse after epinephrine, with an organized narrow complex rhythm at 140, but still with severe shock. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease. of Cardiology AC, Others.
PMID: 30060961 Koller AC, et al. I would rather use a PCAC score to decide on transfer than arrest characteristic (time of CPR, initial rhythm, etc) because we know that all of that data is prone to bias as well. Epub 2016 Jun 28. PMID: 27368428 Elmer J, et al. Ann Emerg Med. Epub 2018 Jul 4. Resuscitation. Here at Pitt, we do not.
Angiography was technically challenging as the patient was receiving CPR, but the cardiologist suspected acute stent thrombosis and initiated cangrelor, although no repeat angiography was able to be obtained. After completing the ACS algorithm with amiodarone and lidocaine, there are diminishing returns on further treatments.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content