This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Author: Brit Long, MD (@long_brit) // Reviewed by Alex Koyfman, MD (@EMHighAK) The American Heart Association (AHA) and Neurocritical Care Society (NCS) released their 2023 Scientific Statement on the criticalcare management of post ROSC patients. Neurocrit Care. Treat seizures if present. 2023 Dec 1. PMID: 38040992.
Welcome back to the tasty morsels of criticalcare podcast. Type 1 is the acute deterioration in kidney function seen in cardiogenic shock from ACS. Welcome back to the tasty morsels of criticalcare podcast. Type 1 is the acute deterioration in kidney function seen in cardiogenic shock from ACS.
Welcome back to the tasty morsels of criticalcare podcast. This week we’re looking at the other ACS, the surgical ACS, the old abdominal compartment syndrome. Read More » Welcome back to the tasty morsels of criticalcare podcast. optimise perfusion.
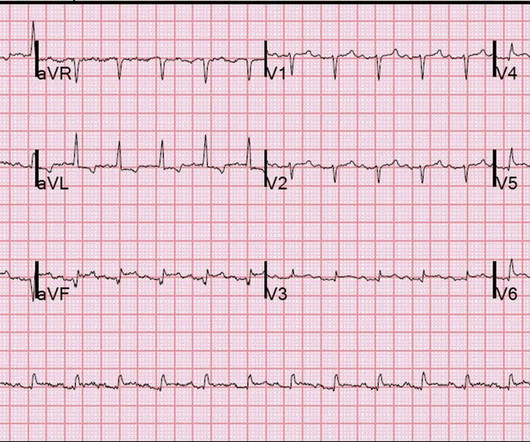
He was rushed by residents into our criticalcare room with a diagnosis of STEMI, and they handed me this ECG: There is sinus tachycardia with ST elevation in II, III, and aVF, as well as V4-V6. ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock. He had this ECG recorded. Are the lungs clear?
Welcome back to the tasty morsels of criticalcare podcast. Critical illness in pregnancy is remarkably rare given the somewhat bonkers system for reproduction that we seem to have evolved over the past million or years. Improved care of complex. Read More » Welcome back to the tasty morsels of criticalcare podcast.
Episode written by Jeff Kott and Tony Breu Kott J, Cooper AZ, Breu AC, Abrams HR. Nephmadness 2024. The Curious Clinicians Podcast. March 4th, 2024. Image source: [link]
Takeaway lessons * If considering ACS in any post-menopausal woman, you should also consider stress cardiomyopathy. Of course, atypical anatomical distributions can also occur in ACS due to distinct anatomy. ACE inhibition). * In general, TCM is a diagnosis of exclusion after ruling out ACS. Find us on Patreon here!
Welcome back to the tasty morsels of criticalcare podcast. Read More » Welcome back to the tasty morsels of criticalcare podcast. doi: 10.21037/acs.2018.03.01. In a breaking from what could only loosely be described as tradition at this point, this podcast is going to be in 2 parts. Ann Cardiothorac Surg.
Article: Vaeli Zadeh A, Wong A, Crawford AC, Collado E, Larned JM. Until then, this study emphasizes the importance of individualized patient care, urging clinicians to weigh guidelines against the specific circumstances and needs of each patient. References: Vaeli Zadeh A, Wong A, Crawford AC, Collado E, Larned JM.
Notoriously elusive, with a high misdiagnosis rate, thoracic aortic dissection (AD) can mimic many conditions, including acute coronary syndrome (ACS, the most common), gastroesophageal reflux disease (GERD), stroke, and spinal-cord compression. The patient is admitted for ACS to a cardiologist who says he will see the patient in the morning.
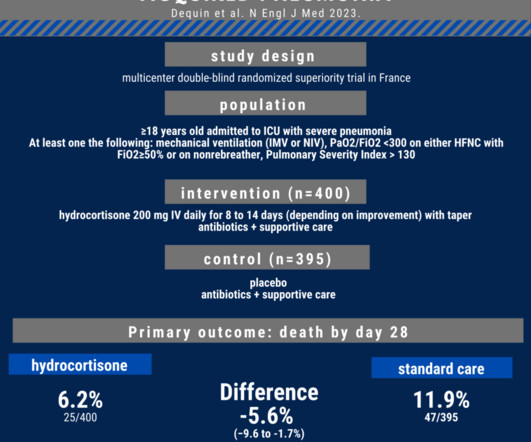
In 2019, the Infectious Disease Society of America recommended against the routine use of steroids in hospitalized patients with community-acquired pneumonia (CAP) while the Society for CriticalCare Medicine recommends steroids in these patients. References: Metlay JP, Waterer GW, Long AC, et al. Intensive Care Med.
This collection of posts features recently published must-know articles. Today we look at the CENSER trial. mL/kg/hr for 2 consecutive hours OR Decrease in serum lactate by more than 10% from initial level Primary outcome – Early norepinephrine group vs. the control group demonstrated higher rates of shock control at 6 hours: 76.1%
While one may argue that nitro really has no mortality benefit in ACS, I have seen patients with CHF present with hyper tension and inferior S-T elevation, in which the providers were scared to even look at the bottle of nitro. References Kimbrell J, Kreinbrook J, Poke D, Kalosza B, Geldner J, Shekhar AC, Miele A, Bouthillet T, Vega J.
This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. Then the patient would have been taken to the criticalcare area with a defibrillator at his side while waiting for the cath lab to be ready. In aVF it is "coved" (upwardly convex). There is ischemic ST depression in V4-V6.
Many conditions outside of acute coronary syndrome (ACS) mimic ST-elevation myocardial infarction (STEMI), but only a handful of cases have reported ST-elevations (STE) in the setting of pancreatic inflammation where underlying ACS was excluded. Journal of CriticalCare. Click to enlarge.) Case Rep Gastroenterol.
No wall motion abnormality This shows that significant ACS can have ZERO WMA!! Then the patient's pain then resolved spontaneously after 2 sublingual nitroglycerine and another ECG was recorded ECG 2 at 16 minutes ST ELEVATION CONSISTENT WITH INJURY, PERICARDITIS, OR EARLY REPOLARIZATION Overread same Smith : The T-waves are now MUCH smaller.
Current can be alternating current (AC) or direct current (DC) with AC typically more dangerous as it is more likely to cause tetanic contractions and increase contact time with the electrical source. 2,3,5 Except for laundry or electrical car outlets (240 V AC), all U.S. household outlets are rated at 120 V AC.
ACS and Aortic Dissection - For ACS and Dissection, the higher CRP levels, the worse prognosis. It is not used to diagnose ACS/Dissection. For diagnostic and prognostic purposes in criticalcare, PCT is superior to CRP and other traditional markers of sepsis. Utility of CRP 1.
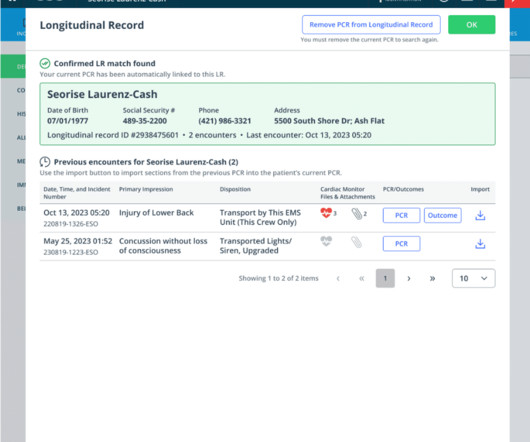
EHR | CriticalCare While rolling out Longitudinal Record in beta, we’ve also continued to expand our CriticalCare offering. Injury Prevention Summary ACS PRQ- Hospice ACS PRQ – Solid organ injuries PtReg: 2.5 Neurosurgeon Response PRQ- 2.12
Sepsis, hyperthyroidism, dehydration, heart failure, ACS, etc). Amiodarone versus Digoxin for Rate Control in Critically Ill Patients with Rapid Atrial Fibrillation or Flutter.” Journal of Emergency and CriticalCare Medicine , vol. Circulation , 5 Nov. 2018, PMID: 30571262 Gritsenko, Diana, et al. 2, 2018, pp.
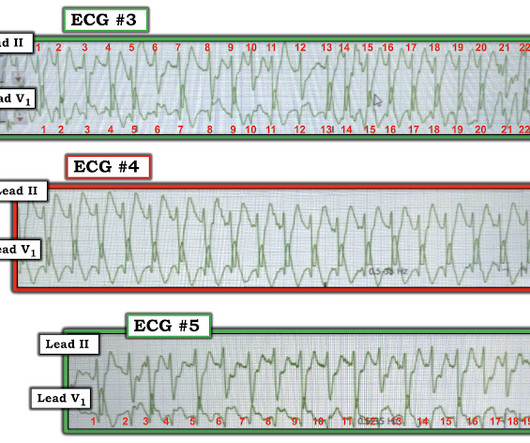
Since ACS is so dynamic, with thrombi forming and lysing continuously, and because the ECG and angiogram are rarely simultaneous, it is probable that de Winter's T-waves are recorded in a window when the artery is barely open. A male in his 30's complained of sudden severe substernal chest pain.
Emmerson AC, Whitbread M, Fothergill RT. P029: A descriptive analysis of defibrillation vector change for prehospital refractory ventricular fibrillation. Canadian Journal of Emergency Medicine. 20(S1):S67. Double sequential defibrillation therapy for out-of-hospital cardiac arrests: The London experience. Resuscitation. 2017;117:97-101.
He was brought to the criticalcare area where these rhythms were seen on the monitor: Wide complex tachycardia with no apparent P-waves, and very irregular Consistent with atrial fibrillation with aberrancy A Regular wide complex tachycardia. Instead, he complained of left chest "itchiness". Learning Points: 1.
In 1999, the TRICC ( Transfusion Requirements in CriticalCare) trial was published in The New England Journal of Medicine. This study took 838 critically-ill patients and randomized them to either a liberal (target Hgb 10-12 g/dL) or conservative ( 7-9 d/gL) transfusion strategy. When Normal Labs Aren’t Necessary.
This EKG was recorded as part of a standing order for criticalcare. Of course this depends on many factors: 1) duration of occlusion, 2) whether full or near occlusion with zero flow or some flow -- the flow in the artery is the critical factor, measured by "TIMI" flow, 3) presence of collateral circulation and others.
Use of inotropes in the criticalcare setting. Crit Care Med 1990; 18:S56. Curr Opin Crit Care 2000; 6:347. Intensive Care Med 2004; 30:597. Intensive Care Med 2012; 38:9. Gordon AC, Mason AJ, Thirunavukkarasu N, et al. MacGregor DA, Smith TE, Prielipp RC, et al. Anesthesiology 2000; 92:338.
We brought the patient into one of our criticalcare rooms and immediately got more history while recording this repeat ECG: The STE in I has greatly diminished or entirely disappeared. Let's zoom in on I and aVL: Lead I (top panel) has less than 1mm of STE. aVL is also less dramatic but still abnormal.
CriticalCare. Goodman AD, Got CJ, Weiss AC. Acute kidney injury due to rhabdomyolysis and renal replacement therapy: a critical review. CriticalCare. Chavez LO, Leon M, Einav S, Varon J. Beyond muscle destruction: a systematic review of rhabdomyolysis for clinical practice. 2016;20(1):135. J Emerg Med.
CriticalCare Medicine 41(12):p A191, December 2013. Chinawa JM, Ubesie AC, Chukwu BF, Ikefuna AN, Emodi IJ. -smoke, high ozone levels, smog) Asthma/reactive airway disease (RAD) Diagnostic criteria 7,8 Respiratory symptoms +/- fever (at least 38.0 C or 100.4 mg/kg, max 4 mg per dose q20-30min) or hydromorphone (0.01-0.02
Darling is a third-year emergency medicine resident at Riverside Regional Medical Center, who will continue her training at the University of Wisconsin with a fellowship in retrieval and criticalcare transport. Kruegel AC, Gassaway MM, Kapoor A, et al. Gold MS, Pottash AC. J Med Chem. 2020;63(1):433-439. J Am Chem Soc.
After completing the ACS algorithm with amiodarone and lidocaine, there are diminishing returns on further treatments. Multidisciplinary criticalcare management of electrical storm. Or was it out of proportion, perhaps worsened by the sympathetic surge? We will never know for certain. link] Jentzer, J. Noseworthy, P.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content