This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. The patient was brought to the ED and had this ECG recorded: What do you think? Then assume there is ACS. See these related cases: Cardiac arrest, defibrillated, diffuse ST depression and ST Elevation in aVR.
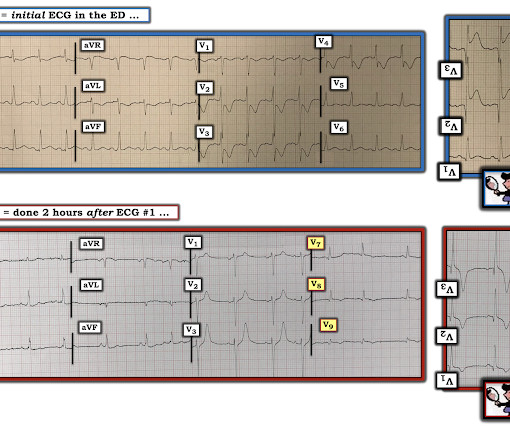
He was defibrillated, but they also noticed that he was being internally defibrillated and then found that he had an implantable ICD. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Here is the initial ED ECG. What do you think?
He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP). She arrives in the emergency department (ED) with decreased level of consciousness and shock.
Here was his initial ED ECG: There is atrial fibrillation with a rapid ventricular response. Does this patient have ACS? Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. He did not have ACS.
This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. VF was refractory to amiodarone, lidocaine, double-sequential defibrillation, esmolol, etc. Then the patient would have been taken to the critical care area with a defibrillator at his side while waiting for the cath lab to be ready.
The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). The arrhythmia spontaneously converted before defibrillation was achieved.
This post will focus on the key parts of the guideline that affect ED evaluation and management. With respect to timing, for cardiac arrest with a shockable rhythm, it may be reasonable to administer epinephrine after initial defibrillation attempts have failed. COR 2b, LOE C-LD. COR 3, No benefit, LOE B-R. COR 2b, LOE B-R.
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. at the time of the ECG.
Submitted by Dr. George Mastoras (Twitter @georgemastoras), written by Jesse McLaren It’s a busy day in the ED when you’re sent another ECG to sign off from a patient at triage. Whereas SCAD is found in ~1-4% of all angiograms performed for ACS — this percentage increases to over 30% in middle-aged women.
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation. CPR was initiated immediately.
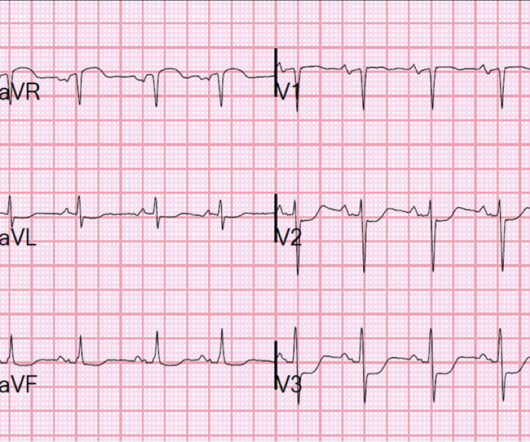
She was never seen to be in ventricular fibrillation and was never defibrillated. She was hypotensive in the ED and her bedside echo showed a normal RV and LV. Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR.
He was found in ventricular fibrillation and defibrillated, then brought to a local ED which does not have a cath lab. Here is the initial ED ECG: This is pretty obviously and inferior posterior OMI, right? He was treated medically for ACS and did not get an angiogram within 72 hours.
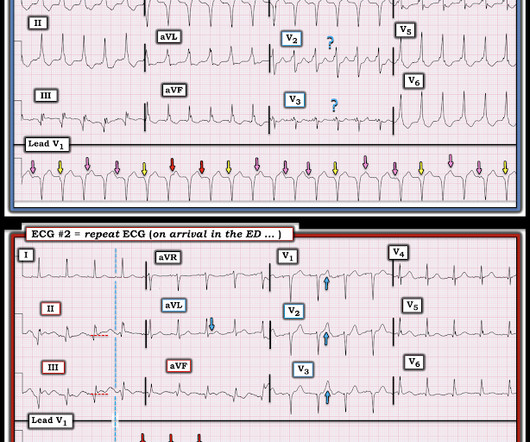
Recall that, in the setting of ACS symptoms, ST depression that are maximal in leads V1-V4 (as opposed to V5 and V6) not attributable to an abnormal QRS complex is specific for OMI. When the ICD was finally interrogated, the syncopal events and shocks correlated with two VF events that were defibrillated successfully.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. She was defibrillated and resuscitated. Most studies examine undifferentiated ACS cohorts, with only a handful providing separate data. References: 1.
A 67-year-old man presents to the emergency department (ED) in cardiac arrest. Multiple attempts at defibrillation, epinephrine, and amiodarone have been unsuccessful. On ED presentation, he is unresponsive and the monitor shows ventricular fibrillation. He was found by bystanders after he collapsed and 911 was called.
But thankfully, when the clinical context is clearly and highly concerning for ongoing ischemia from ACS, this distinction doesn't matter much. Soon after the witnessed occlusion, the patient suffered ventricular fibrillation arrest, from which he was immediately resuscitated with 1 defibrillation. This idea is erroneous.
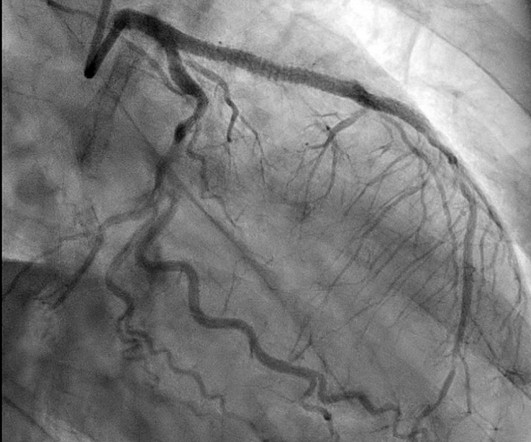
After ruling out for ACS, the patient underwent angiography where he was found to have severe stable disease, which was already known. The patient was then sent to the ED for evaluation not by ambulance but driven to the ED by his wife. This would be approximately 95% of the patient's maximum predicted sinus rate.
He had several older ECGs on file, here are two examples: 6 days prior: 2 months prior: In the context of ACS symptoms, and when able to compare the new vs. old ECG, the top ECG is DIAGNOSTIC of OMI until proven otherwise. Defibrillation was performed, and ROSC was achieved. To Emphasize: Once again the history is KEY.
Whenever I see PVCs with the morphology and axis seen in todays case I always look for signs of AC ( Arrhythmogenic Cardiomyopathy ). See this case for an in-depth discussion of AC and an example of VT and ECG changes associated with this disorder. Arrhythmogenic cardiomyopathy often manifests with PVCs from the RV.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content