This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
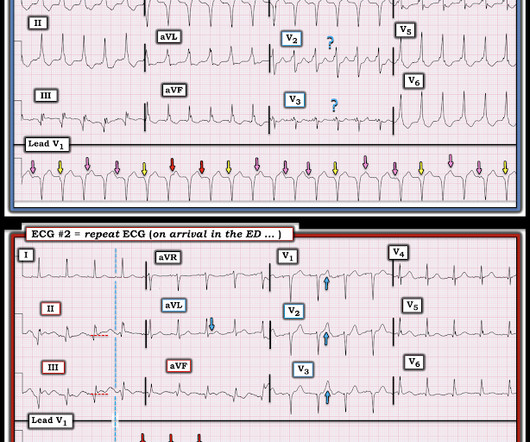
He was resuscitated with chest compressions and defibrillation and 1 mg of epinephrine. ACS would be highly unusual in a young athlete, and given the information on his race bib, one must first suspect that the abnormal ST elevation is due to demand ischemia, not ACS. His initial ECG is shown here.
Assessing the Severity The severity of an electrical burn depends on several factors: the type of current (AC or DC), voltage, the pathway of the current through the body, the duration of contact, and the victim’s overall health. It helps in making informed decisions for the next steps in treatment.
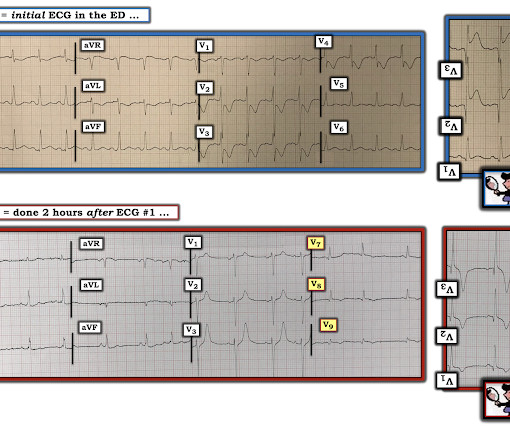
I was texted these ECGs by a recent residency graduate after they had all been recorded, along with the following clinical information: A 50-something with no cardiac history, but with h/o Diabetes, was doing physical work when he collapsed. He was treated medically for ACS and did not get an angiogram within 72 hours.
Recall that, in the setting of ACS symptoms, ST depression that are maximal in leads V1-V4 (as opposed to V5 and V6) not attributable to an abnormal QRS complex is specific for OMI. When the ICD was finally interrogated, the syncopal events and shocks correlated with two VF events that were defibrillated successfully. ng/mL (ULN 0.04).
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. She was defibrillated and resuscitated. Optical coherence tomography, due to its high resolution, may provide additional information [ 10,13 ]. References: 1.
This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. I sent it to 5 of my OMI friends without any clinical information or outcome and all 5 independently responded with exactly the same diagnosis: "reperfused inferior OMI". There is ischemic ST depression in V4-V6. Resuscitative attempts were initiated quickly.
It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation. If this is ACS with Aslanger's pattern , the ST depression vector of subendocardial ischemia (due to simultaneous 3 vessel or left main ACS) is directed toward lead II (inferior and lateral). CPR was initiated immediately.
Remember that the ECG reports what is happening to the myocytes , then you must use that information to make inferences about what the patient needs. One must always be careful when looking for "baseline" ECGs, because the prior ECG on file may have been during another ACS event, as this one clearly was.
After ruling out for ACS, the patient underwent angiography where he was found to have severe stable disease, which was already known. But if you only think that you may be seeing AV dissociation in a regular WCT rhythm then it is best not to include this information in your assessment because it is much more likely than not to misguide you.
Several 200 J shocks did not terminate the VF, so a second defibrillator was applied for double sequential defibrillation with 400 J. She was defibrillated perhaps 25 times. After completing the ACS algorithm with amiodarone and lidocaine, there are diminishing returns on further treatments. SanzRuiz, R., Solis, J., &
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














Let's personalize your content