This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. Then assume there is ACS. See these related cases: Cardiac arrest, defibrillated, diffuse ST depression and ST Elevation in aVR. Cardiac arrest #3: ST depression, Is it STEMI? They started CPR. sodium bicarbonate.
Does this patient have ACS? Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. He did not have ACS. We found that 38% of out of hospital ventricular fibrillation was due to STEMI. Learning Points: 1.
Defibrillation is the treatment of choice in these cases but does not often result in sustained ROSC ( Kudenchuk et al 2006). Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients. Many of these OHCAs are due to ventricular fibrillation or pulseless VT.
He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. VF was refractory to amiodarone, lidocaine, double-sequential defibrillation, esmolol, etc.
He was resuscitated with chest compressions and defibrillation and 1 mg of epinephrine. ACS would be highly unusual in a young athlete, and given the information on his race bib, one must first suspect that the abnormal ST elevation is due to demand ischemia, not ACS. On his bib it stated that he had a congenital heart disorder.
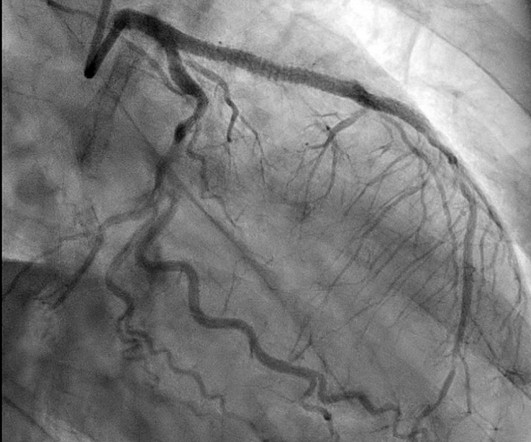
With respect to timing, for cardiac arrest with a shockable rhythm, it may be reasonable to administer epinephrine after initial defibrillation attempts have failed. Consider administering epinephrine after defibrillation in those with shockable rhythms. Editorial Comment : Yes to PCI after arrest with STEMI on ECG.
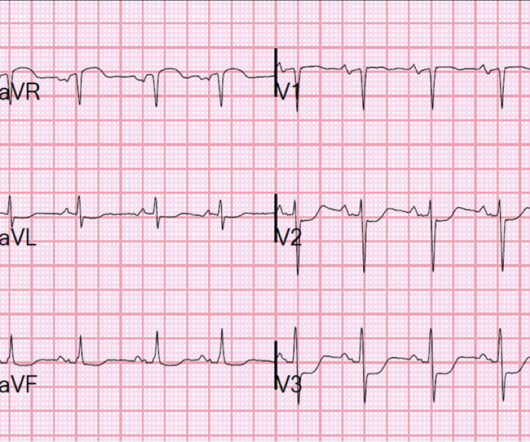
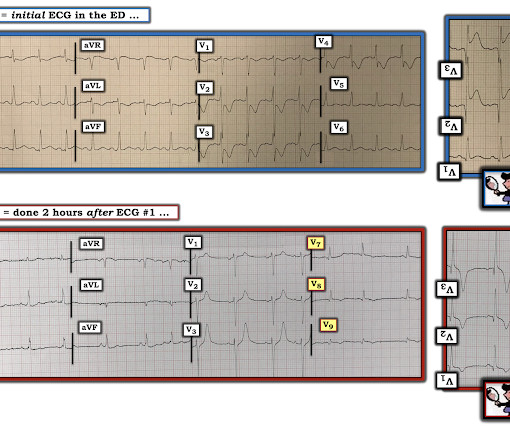
This ECG was read as “No STEMI” with no prior available for comparison. It is true this ECG does not meet STEMI criteria (there is 1.0 The Queen of Hearts sees it of course: Still none of these three ECGs meet STEMI criteria. Do you think we discussed this patient's 2-3 hour delay to reperfusion in our quarterly "STEMI meeting"?
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? He was found in ventricular fibrillation and defibrillated, then brought to a local ED which does not have a cath lab. This is the response he got: Interventionist: "No STEMI, no cath. It is a STEMI equivalent.
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She was immediately intubated during continued compressions, then underwent a 9th defibrillation, which resulted in an organized rhythm at 42 minutes after initial arrest. References : 1.
Discharge ECG showed antero-inferior reperfusion T wave inversion: Had the initial ECG been signed off as “STEMI negative” the patient could have arrested in the waiting room, with a poor cardiac and neurological outcome. For more on this topic — See discussion in the October 24, 2019 and July 31, 2018 posts in Dr.
STEMI , ST-segment elevation acute myocardial infarction ). 1 Initial diagnosis of STEMI ECG Management Recommendation Level of evidence A 12-lead ECG should be interpreted immediately (within 10 minutes) at first medical contact. I B ECG monitoring should start immediately and a defibrillator must be ready.
She was never seen to be in ventricular fibrillation and was never defibrillated. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. BP gradually rose. Kurkciyan et al.
There is a very small amount of STE in some of the anterior, lateral, and inferior leads which do NOT meet STEMI criteria. One must always be careful when looking for "baseline" ECGs, because the prior ECG on file may have been during another ACS event, as this one clearly was. This ECG is highly suspicious for LAD OMI.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. She was defibrillated and resuscitated. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al.
It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation. If this is ACS with Aslanger's pattern , the ST depression vector of subendocardial ischemia (due to simultaneous 3 vessel or left main ACS) is directed toward lead II (inferior and lateral). CPR was initiated immediately.
Recall that, in the setting of ACS symptoms, ST depression that are maximal in leads V1-V4 (as opposed to V5 and V6) not attributable to an abnormal QRS complex is specific for OMI. When the ICD was finally interrogated, the syncopal events and shocks correlated with two VF events that were defibrillated successfully.
But thankfully, when the clinical context is clearly and highly concerning for ongoing ischemia from ACS, this distinction doesn't matter much. Soon after the witnessed occlusion, the patient suffered ventricular fibrillation arrest, from which he was immediately resuscitated with 1 defibrillation.
Several 200 J shocks did not terminate the VF, so a second defibrillator was applied for double sequential defibrillation with 400 J. She was defibrillated perhaps 25 times. After completing the ACS algorithm with amiodarone and lidocaine, there are diminishing returns on further treatments. SanzRuiz, R., Solis, J., &
He had several older ECGs on file, here are two examples: 6 days prior: 2 months prior: In the context of ACS symptoms, and when able to compare the new vs. old ECG, the top ECG is DIAGNOSTIC of OMI until proven otherwise. Unfortunately, the ECG was interpreted as no significant change from prior , "no STEMI"!!
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content