This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Many of the changes seen are reminiscent of LVH with “strain,” and downstream Echo may very well corroborate such a suspicion, but since the ECG isn’t the best tool for definitively establishing the presence of LVH, we must favor a subendocardial ischemia pattern, instead. This was deemed “non-specific” by the ED physicians. Type I ischemia.
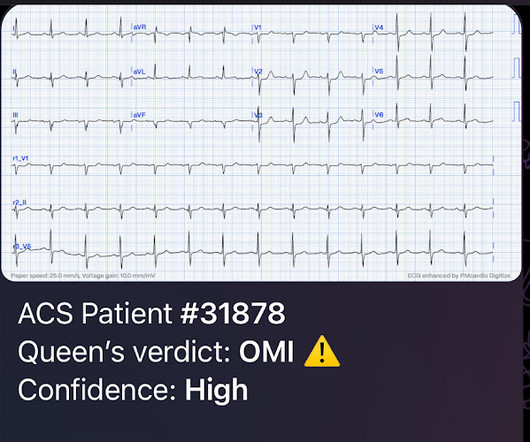
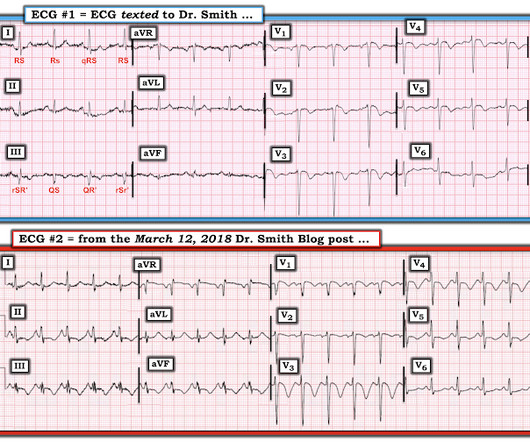
I simply texted back: "Definite posterior OMI." The person I was texting knows implicitly based on our experience together that I mean "Definite posterior OMI, assuming the patient's clinical presentation is consistent with ACS." The patient was a middle-aged female who had acute chest pain of approximately 6 hours duration.
REBEL Cast Ep114 – High Flow O2, Suspected ACS, and Mortality? PMID: 33653685 Clinical Question: Is there an association between high flow supplementary oxygen and 30-day mortality in patients presenting with a suspected acute coronary syndrome (ACS)? Click here for Direct Download of the Podcast Paper: Stewart, RAH et al.
Then assume there is ACS. Confirmation of sinus tachycardia should be easy to verify when the heart rate slows a little bit ( as the patient's condition improves ) — allowing clearer definition between the T and P waves. The ST depression usually resolves, or is clearly resolving (getting much better).
RBBB + LAFB in the setting of ACS is very bad. Some patients have baseline RBBB with LAFB, but in patients with likely ACS, these are associated with severe infarction with cardiac arrest, cardiogenic shock or impending shock. Patients with ACS and RBBB/LAFB usually have a left main vs. proximal LAD. Learning Points: 1.
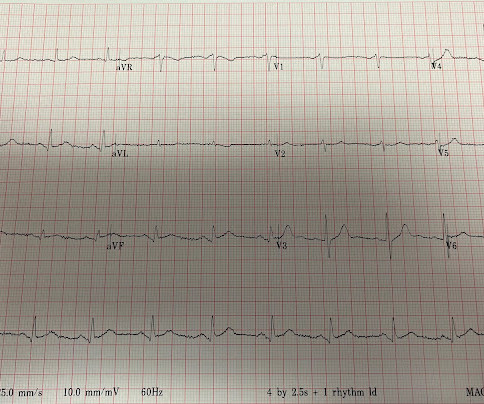
This was texted to me from a former resident, while working at a small rural hospital, with the statement: "I can’t convince myself of anything here, but he’s a 63-year-old guy with prior stents and a good story for ACS." Chest pain or discomfort) What do you think? Here was my response: "Suspicious for inferior posterior OMI.
The ECG does not show any definite signs of ischemia. The patient presented due to chest pain that was typical in nature, retrosternal and radiating to the left arm and neck. He denied any exertional chest pain. The below ECG was recorded. It is unclear if the patient was pain free at this time.
In an attempt to clarify language, a consensus definition was developed. The definition requires the following three components: An end QRS notch (sometimes called a J wave) or slur, in the case of a slur it must lie entirely above the isoelectric baseline The peak amplitude of the notch or slur should be ≥ 0.1 ECG 2 What do you think?
There were zero patients in this study with a "normal" ECG who had any kind of ACS! Over the years — various definitions have been proposed for what should constitute a " significant " Q wave , based on width and/or depth of the Q wave. So this study is actually worthless.
These results are not definitive, but considering the rarity of demyelination, and the magnitude of the mortality results, this should probably influence clinical practice until we get the proper RCTs. WOMAN are so negative WOMAN-2 Trial Collaborators. Emerg Med J. 2019 Jan;36(1):2-3. doi: 10.1136/emermed-2018-208151. Epub 2018 Oct 25.
Therefore, this does not meet the definition of myocardial infarction ( 4th Universal Definition of MI ), which requires at least one troponin above the 99% reference range. You can see the deficiency of the definition of MI. This is subtle — but it is definitely present. But maybe not. Mokhtari et al. JACC 2016;67:1531.
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. Smith : This is ACS even if the troponin returns normal, and the first troponin especially might return normal. It is accelerated angina, which is by definition not stable.
Thus, this does NOT meet STEMI criteria (though, as of 2022, it is a formal "STEMI equivalent", assuming everyone agrees that this is de Winter morphology, for which there is currently no objective definition). Everywhere I'm aware of (only about 5 systems), the ECGs are not even recorded in the "STEMI database." What a farce.
1, 2] The most clinically useful definition to account for this entire constellation is intraventricular conduction delay. Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion. second (ie, with a pure fascicular VT) — so How can you NOT count 0.11
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Most studies examine undifferentiated ACS cohorts, with only a handful providing separate data. References: 1.
Because the most severe LAD OMIs can cause ischemic failure of the RBB and LAF, any patient with ACS symptoms and new RBBB and LAFB with any concordant STE has LAD OMI until proven otherwise. Post cath EF was estimated at 15% with severe global hypokinesis, and akinesis of the apex. Long term outcome is unavailable.
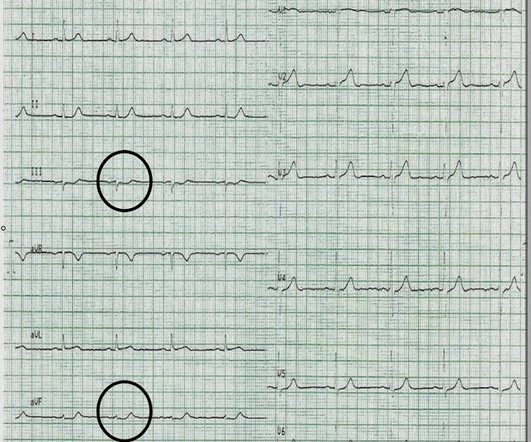
This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. Suppose the OMI had been recognized, or suppose another ECG had been recorded and it showed definite OMI. The 3rd inferior lead ( = lead II ) — shows definite ST-T wave flattening. In aVF it is "coved" (upwardly convex).
Click here for Direct Download of the Podcast Paper: Aykan AC et al. PMID: 23102885 Aykan AC et al. Because the lungs receive 100% of cardiac output, it has been hypothesized that a lower dose of thrombolytic therapy may still be effective with a better safety profile [3][4]. Clin Exp Emerg Med 2023. JACC Cardiovasc Interv 2018.
Similarly, the OMI paradigm respects ACS as a dynamic process in which ECG changes reflect the phase of myocardial injury and risk stratify which patients may benefit from emergent PCI. Although tiny in size — the BLUE arrows highlight definite ST elevation in leads I and aVL. In fact, use of antidyrhythimcs (e.g., Leave it alone.
When Pendell and I are coding ECGs for the Queen's training, this is one category: "Definite ischemia, difficult to differentiate between posterior OMI and subendocardial ischemia." In our opinion it should not be given in ACS unless you are committed to the cath lab. In my opinion, I think it looks more like subendocardial ischemia.
80%) and definitely too much for hour to hour. However, the Definition of MI requires at least one value above the 99th percentile, which for a male is 34 ng/L (16 ng/L for women). Thus, these troponins are very concerning for ACS, and subsequent ones will probably be diagnostic of acute MI. of the time.
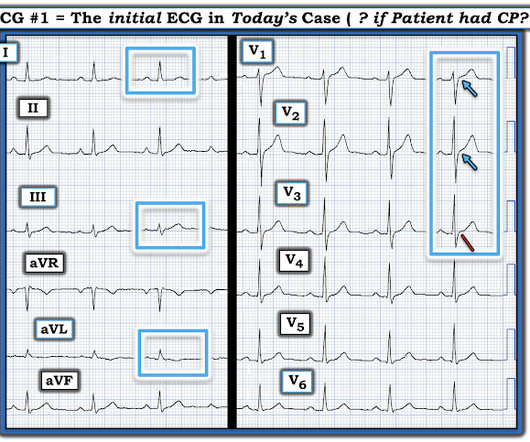
Definition: Technically, for the tracing in ECG #1 to truly “qualify” as Wellens’ Syndrome — there should be no CP at the time the ECG is recorded. However, in the chest leads — there has definitely been evolution , in that ST segments are more coved and slightly more elevated in virtually all chest leads.
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Link to abstract Link to full text 2) Use of Morphine in Non-STE-ACS is independently associated with mortality, at odds ratio of 1.4
This week we’re looking at the other ACS, the surgical ACS, the old abdominal compartment syndrome. This week we’re looking at the other ACS, the surgical ACS, the old abdominal compartment syndrome. These are all very nice and should all be reflected upon and followed when appropriate in your ACS.
However , this patient is having chest discomfort, and by definition then she should be considered not to be stable. Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? If the patient is hemodynamically stable, iv amiodarone could be considered in such a clinical situation. Is this: 1.
Because there was proven thrombus (ACS) but the troponin never went above the 99% reference range (and therefore cannot be called MI -- definition of MI requires rise and/or fall of troponin with at least one value above the 99% reference range), this is UNSTABLE ANGINA with ST Elevation.
There is perhaps a tiny J-wave in several of the QRS complexes in V3, but it would not be enough to definitively say there is a J-wave. Lead aVL, for example, has a definite J-wave. link] He was admitted to the cardiology unit for serial troponin measurements and concern for possible ACS. Stat echo would also be helpful.
Apple Podcasts , Spotify , Listen Here Resuscitative endovascular balloon occlusion of the aorta (REBOA) is a minimally invasive way of providing resuscitative aortic occlusion in severe hemorrhage to gain temporary hemorrhage control as a bridge to definitive procedures. ” As a result, Jansen et al.
Moreover, what I call "domed" T-wave inversion in V1-V3 is typical for acute PE and NOT typical of ACS (i.e., Moreover, T-wave inversion in V1-V3 due to ACS is typically seen in reperfusion states when the patient is symptom free. Wellens'), presumably because the source of the T-wave inversion is RV strain, not LV ischemia.
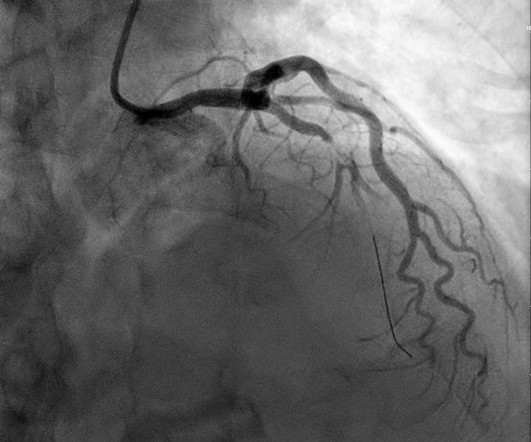
Here is an article I wrote: Updates on the ECG in ACS. Was this: 1) ACS with ischemia and spontaneous reperfusion? The patient was taken for an angiogram and had an 80% LAD lesion, but it could not be definitely determined whether this was an acute thrombotic lesion or a chronic stable lesion.
ACS then becomes less likely. BOTTOM Line: There clearly is enough on this initial ECG to support Dr. Nossen's concern that a definitive diagnosis needed to be made on this young man with new, persistent chest pain. On arrival patient was slightly tachycardic. HR about 90-100/min. Other vital signs normal. at ~100/minute ).
Some providers were worried about ACS because of this ECG. My answer alleviated their concern for ACS and no further workup was done for ACS. showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS. Kosuge et al.
But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Dialysis patients have a high rate of ACS without chest pain and high rate of delayed diagnosis and delayed reperfusion 2.
This pattern occurs regardless of whether the cause is ACS (decreased supply) or any other cause of decreased supply or increased demand. You must understand that this pattern does not differentiate ACS from other causes of supply/demand mismatch. Figure-1: The initial ECG in today's case. (
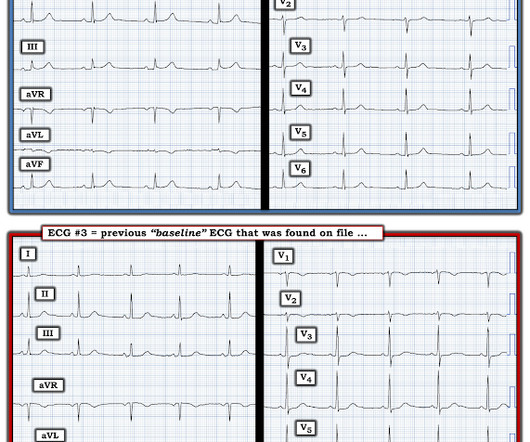
Despite the seemingly worrisome ST-T wave changes on serial tracings shown in Figure-1 — an acute event was definitively ruled out by 4 consecutive negative hs troponins — with further support provided by an Echo showing excellent LV function without wall motion abnormality. So they looked into the patient's chart. Some patients do this.
The patient has ACS by history, active pain, and an elevated troponin. By definition , this is acute myocardial infarction, the only question now is the etiology. It is impossible to overstate the importance of putting the ECG and troponin into the context of the clinical history. Smith : at this point, the ECG becomes irrelevant.
Episode 107: Eclampsia Definition: Severe hypertensive disease of pregnancy (HDP) with new onset tonic-clonic, focal, or multifocal seizures or unexplained altered mental status in a patient who is pregnant or postpartum and there’s no other causative etiologies. Wilkerson RG, Ogunbodede AC. 2022;226(2S):S1237-S1253.
See this study showing an association between morphine and mortality in ACS: Use of Morphine in ACS is independently associated with mortality, at odds ratio of 1.4. See this case: A man his 50s with chest pain. What happens when you treat with morphine rather than with reperfusion?
If you like the types of questions we answer on The Curious Clinicians, you’ll definitely want to check that out and subscribe. Listen to the episode [link] Credits & Citatio n Episode written by Avi Cooper Show notes written by Giancarlo Buonomo and Avi Cooper Audio edited by Clair Morgan of nodderly.com Cooper AZ, Breu AC, Abrams HR.
Therefore, even with a normal or non-diagnostic ECG, a 50 year old male patient should undergo serial ECGs and troponins and be admitted to a monitored bed until MI or ACS can be ruled out. There is no way to tell the difference between GI etiology of chest pain and MI. This is obviously a very big topic in itself.
REBOA increased deaths due to bleeding at three hours and 90 days and substantially delayed time to definitive haemorrhage control. REBOA increased deaths due to bleeding at three hours and 90 days and substantially delayed time to definitive haemorrhage control. c) Or, do both? Trauma Surg Acute Care Open.
SCAD isn’t rare, especially in women Historically SCAD had been identified in 22% of ACS cases in women. Pregnancy is not a common cause of SCAD When ACS occurs in the peripartum period, SCAD is responsible in 43% of cases. Lead-by-lead comparison of ECGs #1 and #2 shows definite improvement.
3) RV Failure leads to hypotension but NOT pulmonary edema (unlike LV failure) 4) Repeat ECGs, right sided ECG and bedside echo may be helpful in making a diagnosis of ACS. Lead aVL is definitely not normal. Smith's book : Learning points: 1) OMI can be very subtle and RV infarction may manifest poorly on the standard ECG.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content