This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
At the time of ED arrival he was alert, oriented, and verbalizing only a headache with a normalized BP. The ED activated trauma services, and a 12 Lead ECG was captured. This was deemed “non-specific” by the ED physicians. Thus, the ED admission ECG changes cannot be blamed on LVH. The fall was not a mechanical etiology.
These results are not definitive, but considering the rarity of demyelination, and the magnitude of the mortality results, this should probably influence clinical practice until we get the proper RCTs. The protocol used the ADD score, a POCUS echo protocol and D-dimer to try and exclude AAS in the ED. Did they pick a heap of PEs?
But this time the Queen gets it wrong (thinks it is not OMI): There were runs of VT: Tha patient arrived in profound shock and had an ED ECG: Now there is some evolution to include the ST elevation (rather than ST depression) in V4-V6. RBBB + LAFB in the setting of ACS is very bad. Posterior and high lateral OMI. Learning Points: 1.
The patient was brought to the ED and had this ECG recorded: What do you think? Then assume there is ACS. Confirmation of sinus tachycardia should be easy to verify when the heart rate slows a little bit ( as the patient's condition improves ) — allowing clearer definition between the T and P waves. sodium bicarbonate.
I simply texted back: "Definite posterior OMI." The person I was texting knows implicitly based on our experience together that I mean "Definite posterior OMI, assuming the patient's clinical presentation is consistent with ACS." The patient was a middle-aged female who had acute chest pain of approximately 6 hours duration.
However, many institutions’ surgical teams still require or request a formal study over a bedside exam, likely due to a lack of confidence in the accuracy of POCUS, resulting in longer ED stays. ACS surgeons appeared to select surgery as their initial choice substantially more frequently than other subspecialties.
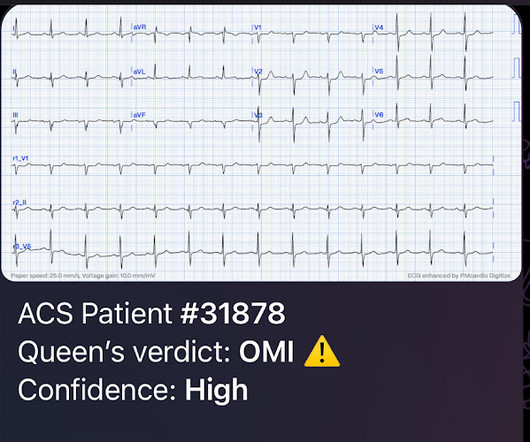
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (ret) @DidlakeDW Expert commentary and peer review by Dr. Steve Smith [link] @smithECGBlog A 57 y/o Female with PMHx HTN, HLD, DM, and current use of tobacco products, presented to the ED with chest discomfort. A 12 Lead ECG was captured on her arrival.
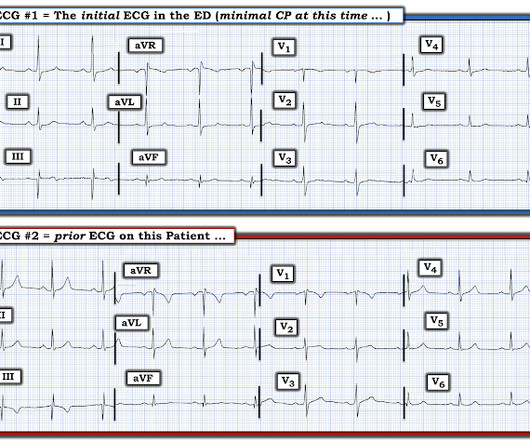
There were zero patients in this study with a "normal" ECG who had any kind of ACS! Figure-1: I've labeled the initial ECG in the ED. KEY Point: All patients who present to the ED for new CP should promptly have a triage ECG recorded, that is then immediately interpreted by the ED physician.
Also known as Facilitated intubation (FI), the use of intubating with only a sedative was an accepted alternative intubation technique prior to those definitive studies in the late 1990s but quickly was abandoned for RSI in all emergent endotracheal intubations (ETI) (8,9). To date, ketamine has been the agent of choice (12).
Cardiology consult note written around that time documents that "Pain improved with NTG, morphine in ED but still present." In an attempt to clarify language, a consensus definition was developed. mV in 2 or more contiguous leads (excluding V1-V3) The QRS duration should be < 120 ms This definition is not perfect.
[link] Case continued She arrived in the ED and here is the first ED ECG. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. I don't know if her pain was getting better or not.
Because the most severe LAD OMIs can cause ischemic failure of the RBB and LAF, any patient with ACS symptoms and new RBBB and LAFB with any concordant STE has LAD OMI until proven otherwise. So the cath lab was activated. Post cath EF was estimated at 15% with severe global hypokinesis, and akinesis of the apex.
1, 2] The most clinically useful definition to account for this entire constellation is intraventricular conduction delay. Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion. second (ie, with a pure fascicular VT) — so How can you NOT count 0.11
This is acute ACS, but it almost always seen in a pain free state. An ED ECG, if recorded with pain, should show LAD OMI. So this ECG was immediately recorded: Indeed, as predicted, a patient with previous Wellens' waves who now definitely has chest pain has acute Occlusion, with new ST elevation in I, aVL, V2-V5.
Prior episodes had simply resolved after brief symptoms, but the current episode had lasted for 2 hours without improvement, so she presented to the ED. At triage she stated her pain is still persistent, but it is mildly improved compared to when she decided to come to the ED. No diaphoresis or vomiting.
This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. Suppose the OMI had been recognized, or suppose another ECG had been recorded and it showed definite OMI. The 3rd inferior lead ( = lead II ) — shows definite ST-T wave flattening. In aVF it is "coved" (upwardly convex).
However , this patient is having chest discomfort, and by definition then she should be considered not to be stable. Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? This patient presented to the ED “after a couple of days of chest discomfort”. Is this: 1.
Episode 107: Eclampsia Definition: Severe hypertensive disease of pregnancy (HDP) with new onset tonic-clonic, focal, or multifocal seizures or unexplained altered mental status in a patient who is pregnant or postpartum and there’s no other causative etiologies. ED Evaluation: Assessment focuses on looking for complications and mimics.
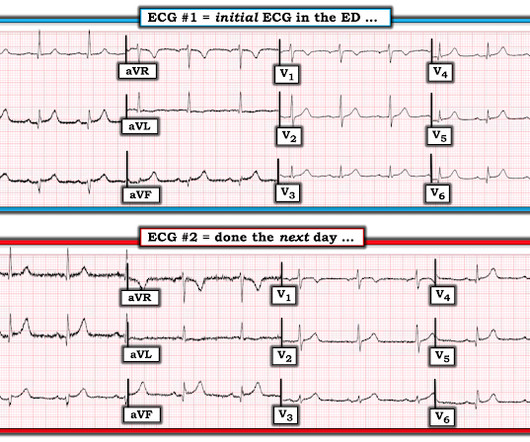
Here is the first ED ECG recorded, now pain free after sublingual Nitro: There is what appears to be a reperfusion T-wave in I and aVL. The 3rd tracing in Figure-1 was the initial ED ECG — obtained at a time when the patient's CP had resolved. Shortly thereafter, on arrival in the ED — ECG #3 was recorded. Some patients do this.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. In our opinion it should not be given in ACS unless you are committed to the cath lab.
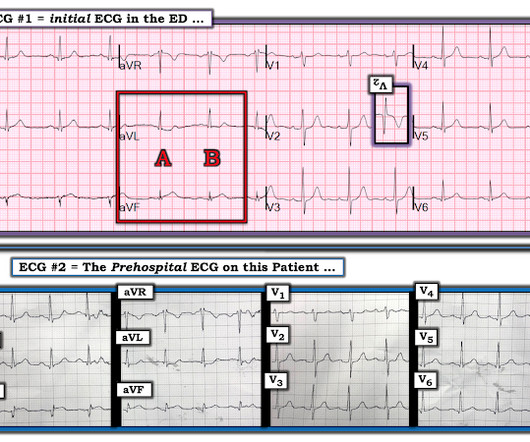
Jerry Jones commented: "Any ST depression on the ECG of a patient with chest pain credible for ACS represents a reciprocal change until proved otherwise." For clarity — I show in Figure-1 the i nitial E CG obtained in the ED ( = E CG # 1 ) — together with the p rehospital E CG that I have pieced together ( = E CG # 2 ).
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Link to abstract Link to full text 2) Use of Morphine in Non-STE-ACS is independently associated with mortality, at odds ratio of 1.4
Because there was proven thrombus (ACS) but the troponin never went above the 99% reference range (and therefore cannot be called MI -- definition of MI requires rise and/or fall of troponin with at least one value above the 99% reference range), this is UNSTABLE ANGINA with ST Elevation. After all, there is no S wave in lead V3.
Written by Jesse McLaren A 75 year-old patient with diabetes and end stage renal disease was sent to the ED after dialysis for three days of nausea, vomiting, loose stool, lightheadedness and fatigue. But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. Below is the 15 lead ECG.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Around 19 hours later, he experienced the same pain, which prompted his presentation to the ED.
Sent by anonymous, written by Pendell Meyers A man in his late 40s presented to the ED with concern for allergic reaction after accidentally eating a potential allergen, then developing an itchy full body rash and diarrhea. In the ED he received methylprednisolone, diphenhydramine, and epinephrine for possible anaphylaxis.
She arrived in the ED 37 minutes after 911 was called, with continuing CPR. Here is an article I wrote: Updates on the ECG in ACS. Was this: 1) ACS with ischemia and spontaneous reperfusion? Fine ventricular fibrillation She received 2 mg epinephrine, 150 mg amiodarone and underwent chest compressions with the LUCAS device.
All you know, back in ED, is that the ETA is 10 minutes, and there is a single stab wound to the chest. The ODP is caught up leaving theatres and has not yet made it down to ED. Back in ED with Ranulf, and pack two has gone through. The trauma call goes out. Would you like a pigtail catheter or a surgical chest tube?
It has been well over a year since the controversial publication of the Agency for Healthcare Research and Quality (AHRQ) report on diagnostic errors in the emergency department (ED). percent of ED visits resulted in preventable death as result of diagnostic error. Available from: [link] Newman-Toker DE, Nassery N, Schaffer AC, et al.
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chest pain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
To the ED providers, the patient denied CP, SOB, or drug use. This is the ED bedside echo, recorded during ST elevation: Parasternal short axis shows huge concentric LVH. I remained unconvinced that this was due to ACS. My interpretation: LVH with secondary ST-T abnormalities, exaggerated by stress, not a STEMI.
link] A 30 year-old woman was brought to the ED with chest pain. SCAD isn’t rare, especially in women Historically SCAD had been identified in 22% of ACS cases in women. Pregnancy is not a common cause of SCAD When ACS occurs in the peripartum period, SCAD is responsible in 43% of cases. This is written by Brooks Walsh.
Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. Here is the ED ECG on arrival: Less STE/STD Provider's Clinical Impression: "findings concerning for myocardial infarction, likely proximal LAD or Left main."
One of the most hair-raising presentations to the emergency department (ED) can be massive hemoptysis with respiratory failure. The definition of massive hemoptysis is variable across publications with expectorated blood volumes ranging from 100 to 1,000 mL per 24 hours, as these volumes are difficult to estimate for any given patient.
Background Information: Atrial fibrillation with rapid ventricular rate (RVR) is one of the many tachydysrhythmias we encounter in the Emergency Department (ED). The average time to control HR in the IV amiodarone was 1.7h, which is usually the average time for disposition from the ED. Paper: Mason JM, et al.
The patient vomited once and given the more intense pain decided to come to the ED. Smith comment: We have shown that use of opiates is associated with worse outcomes in ACS: Bracey, A. 2-hour hsTn: 615 ng/L; bedside ED echo (without contrast) did not show a clear wall motion abnormality (WMA). Abstract 556.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. Most studies examine undifferentiated ACS cohorts, with only a handful providing separate data. Do not let your consultants diagnose takotsubo when it is clearly OMI.
She was hypotensive in the ED and her bedside echo showed a normal RV and LV. Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR. BP gradually rose.
They gave him 2 nitroglycerine and transported to the ED. In the ED, the patient was "moaning, writhing in bed, and clutching his chest." Here is the first ED ECG (there was no previous ECG on file for comparison): Sinus rhythm and LVH There is some (less than 1 mm) of STD in V3 and V4. There is no significant ST Elevation.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. I cannot be anything else.
There is definite STE inferior and lateral but it just doesn't look like true positive STE to me. I wouldn't activate the lab for this EKG alone, but if the patient is clinically compatible with ACS you could call a heart alert. If I had known there was no definite chest pain or pressure this would have been slightly more confident.
CT Coronary angiogram is usually used to make ACS much less likely in the context of a patient who is ruled out for acute MI by troponins. The most remarkable finding on ECG #1 — is fairly shallow but-definitely-present T wave inversion in leads V1-thru-V5. Transient STEMI is at high risk of re-occlusion.
The best study was an ED study that showed that about 7% of patients with chest pain and new LBBB in the ED were diagnosed with acute MI. Lack of association between LBBB and Acute MI in symptomatic ED patients. This patient presented to the ED with complete LBBB. Chang et al. 21, 2015 post by Dr. Smith ).
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content