This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
David Didlake @DidlakeDW EMS personnel responded to the residence of an 81 y/o Male with syncope. Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates). His spouse had called 911 after she heard a loud “thud” in the adjacent room. Type I ischemia.
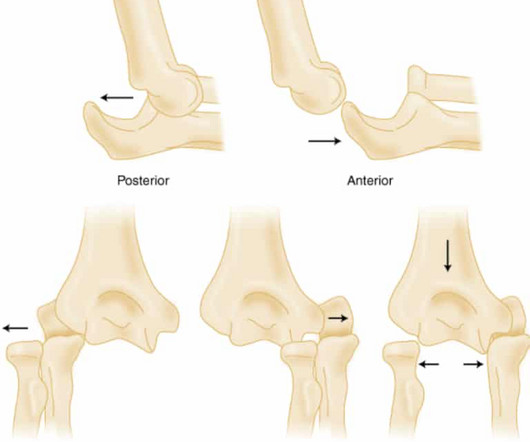
PMID: 32644703 Robinson PM, Griffiths E, Watts AC. PMID: 27227986 Glover NM, Black AC, Murphy PB. PMID: 31082090 Post Peer Reviewed By: Anand Swaminathan MD, MPH (Insta @EMSwami) The post Elbow Dislocations appeared first on REBEL EM - Emergency Medicine Blog. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. 2023 Nov 5.
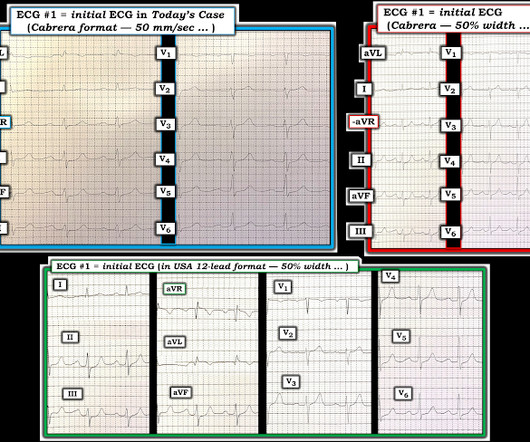
EMS arrived and found him in Ventricular Fibrillation (VF). Then assume there is ACS. Confirmation of sinus tachycardia should be easy to verify when the heart rate slows a little bit ( as the patient's condition improves ) — allowing clearer definition between the T and P waves. They started CPR. He was defibrillated into VT.
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. Smith : This is ACS even if the troponin returns normal, and the first troponin especially might return normal. It is accelerated angina, which is by definition not stable.
1, 2] The most clinically useful definition to account for this entire constellation is intraventricular conduction delay. Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion. second (ie, with a pure fascicular VT) — so How can you NOT count 0.11
EMS obtained the following vital signs: pulse 50, respiratory rate 16, blood pressure 96/49. It appears EMS obtained two EKGs, but unfortunately these were not saved in the medical record. The EMS crew was only BLS certified, so EKG interpretation is not within their scope of practice.
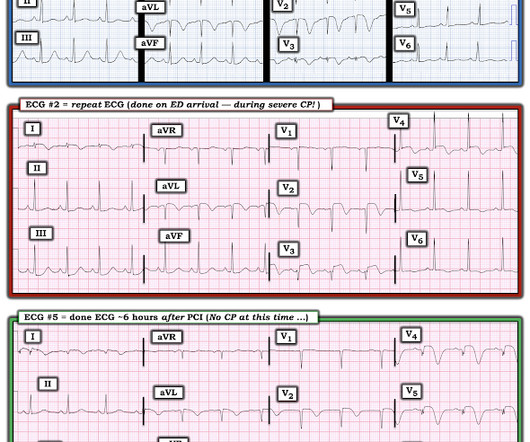
EMS arrived — and recorded 2 ECGs. I added dotted RED lines at the transition between leads V2 and V3 in both of the prehospital ECGs to highlight this common featur e in EMS tracings — in which large QRS complexes will often be truncated. 14 minutes later — ECG #2 was recorded by EMS. So they looked into the patient's chart.
When Pendell and I are coding ECGs for the Queen's training, this is one category: "Definite ischemia, difficult to differentiate between posterior OMI and subendocardial ischemia." In our opinion it should not be given in ACS unless you are committed to the cath lab. He was diagnosed as NSTEMI.
ACS surgeons appeared to select surgery as their initial choice substantially more frequently than other subspecialties. ACS surgeons would have sent 6/43 patients for ERCP or MRCP (14%), whereas surgical oncologists would have sent a higher percentage of patients for ERCP or MRCP (7/18 or 38.9%).
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chest pain. Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS.
This is acute ACS, but it almost always seen in a pain free state. So this ECG was immediately recorded: Indeed, as predicted, a patient with previous Wellens' waves who now definitely has chest pain has acute Occlusion, with new ST elevation in I, aVL, V2-V5. An ED ECG, if recorded with pain, should show LAD OMI.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. Do not let your consultants diagnose takotsubo when it is clearly OMI.
This could have biased the results in favor of amiodarone as we’ve covered this before on REBEL EM before The IV amiodarone group required less additional HR control agents to control increased heart rate. Sepsis, hyperthyroidism, dehydration, heart failure, ACS, etc).
Only if you are uncertain about the diagnosis of ACS. The EM physicians activated their "heart alert" pathway, which immediately summons the cardiology fellow to bedside to evaluate for potential emergent cardiac catheterization lab activation. Bedside POCUS revealed inferior wall motion abnormality (images not available).
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chest pain, weakness and nausea. En route, EMS administered aspirin 325mg by mouth, but withheld nitroglycerin due to initial hypotension. Answer below in the still shot.
He had multiple cardiovascular risk factors and the EM physician strongly suspected ACS. A millimeter definition of acute STEMI should not be needed to justify the need for prompt cardiac catheterization. Written by Pendell Meyers A male in his early 50s presented with waxing and waning chest pain starting at rest.
The provider, and former HCMC EM resident, was exceedingly perceptive and able to accurately diagnose LAD occlusion from this very subtle ECG. If a patient has symptoms of ACS, and they are persistent, and a diagnostic troponin, then cath lab activation is indicated. Often this would include resolution of the LBBB.
The patient contacted EMS after a few hours of chest pain that started 5:30 AM. There is slight but definite ST elevation with an inverted T wave in lead aVL. Learning Points : Serial ECG are very valuable when it comes to identifying a dynamic process such as ACS. He is otherwise healthy. The ECG is live fed to our institution.
REBEL Cast Ep114 – High Flow O2, Suspected ACS, and Mortality? PMID: 33653685 Clinical Question: Is there an association between high flow supplementary oxygen and 30-day mortality in patients presenting with a suspected acute coronary syndrome (ACS)? Click here for Direct Download of the Podcast Paper: Stewart, RAH et al.
Written by Pendell Meyers A man in his 40s called EMS for acute chest pain that awoke him from sleep, along with nausea and shortness of breath. Because the most severe LAD OMIs can cause ischemic failure of the RBB and LAF, any patient with ACS symptoms and new RBBB and LAFB with any concordant STE has LAD OMI until proven otherwise.
RBBB + LAFB in the setting of ACS is very bad. Some patients have baseline RBBB with LAFB, but in patients with likely ACS, these are associated with severe infarction with cardiac arrest, cardiogenic shock or impending shock. Patients with ACS and RBBB/LAFB usually have a left main vs. proximal LAD. Learning Points: 1.
About 2 hours later the patient arrived at a PCI-capable center and repeat ECG was obtained: The transferring EMS crew noted “runs of VT” during transport. Similarly, the OMI paradigm respects ACS as a dynamic process in which ECG changes reflect the phase of myocardial injury and risk stratify which patients may benefit from emergent PCI.
Click here for Direct Download of the Podcast Paper: Aykan AC et al. PMID: 23102885 Aykan AC et al. appeared first on REBEL EM - Emergency Medicine Blog. Because the lungs receive 100% of cardiac output, it has been hypothesized that a lower dose of thrombolytic therapy may still be effective with a better safety profile [3][4].
Also known as Facilitated intubation (FI), the use of intubating with only a sedative was an accepted alternative intubation technique prior to those definitive studies in the late 1990s but quickly was abandoned for RSI in all emergent endotracheal intubations (ETI) (8,9). References: Heffner AC et al. We don’t want to go backwards!
REBOA increased deaths due to bleeding at three hours and 90 days and substantially delayed time to definitive haemorrhage control. REBOA increased deaths due to bleeding at three hours and 90 days and substantially delayed time to definitive haemorrhage control. c) Or, do both? 2014 Sep;45(9):1287-95. Trauma Surg Acute Care Open.
The definition of massive hemoptysis is variable across publications with expectorated blood volumes ranging from 100 to 1,000 mL per 24 hours, as these volumes are difficult to estimate for any given patient. Bourke Tillmann and Scott Weingart for their expertise on the EM Cases podcast that inspired this column. 2021;42(1):145-159.
Garabon JJW, Gunz AC, Ali A, Lim R. EMS Use and Success Rates of Intraosseous Infusion for Pediatric Resuscitations: A Large Regional Health System Experience. Based on this study, further prospective research with more stringent outcome definitions may help to expand and clarify (e.g. Prehosp Emerg Care. 2023;27(2):221-226.
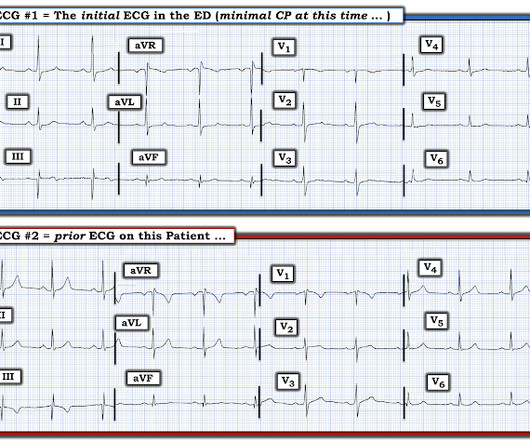
One must always be careful when looking for "baseline" ECGs, because the prior ECG on file may have been during another ACS event, as this one clearly was. The EM physicians at the outside hospital appropriately activated the cath lab transfer protocol but that order was subsequently negated by others.
Likely due to different definitions for hypotension and adverse/major critical events, but the numbers remain higher than we would ever like — Kinda scary when you think about it. Dr. Jarvis of The EMS Lighthouse Project podcast also covers this paper in detail here: [link] ^^^ I highly recommend listening! Is there a targeted SI?
She did not receive any opioids (which would mask her pain without affecting any underlying ACS). Lead I has a definitively hyperacute T-wave without STE. J of National Association of EMS Physicians 2014. She was asymptomatic at the time of this ECG recorded on arrival to our ED: What do you think? II, III, aVF, and V6 have STD.
We’ll keep it short, while you keep that EM brain sharp. A 17-year-old girl, in moderate distress, is brought in by EMS after a motor vehicle collision. EMS reports that she was “pinned” underneath the dashboard, and it took several hours to extricate her. Goodman AD, Got CJ, Weiss AC. J Emerg Med. 2014;46(2):313-319.
Authors: Christian Gerhart, MD (EM Resident Physician, Washington University School of Medicine, St. Louis, MO); Jessica Pelletier, DO (EM Education Fellow, Washington University School of Medicine, St. We’ll keep it short, while you keep that EM brain sharp. A 64-year-old male presents by EMS to the ED with shortness of breath.
Authors: Rachel Kelly, MD ( EM Resident Physician, Stony Brook University Hospital); Robert Nocito, MD (EM Attending Physician, Stony Brook University Hospital) // Reviewed by: Jessica Pelletier, DO (EM Education Fellow, Washington University in St. 11) Webb RK, Ralston AC, Runciman WB. proning patients, ECMO) (12).
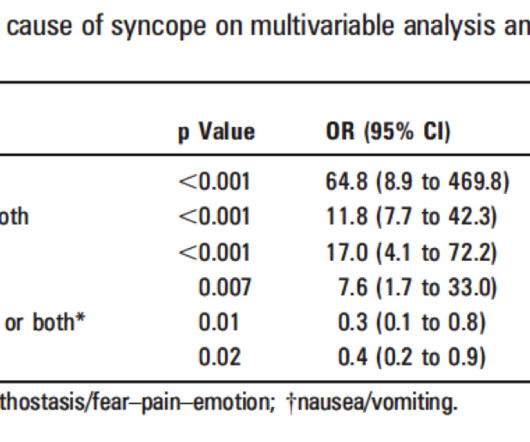
Approach to Syncope Syncope definition: Brief loss of consciousness with loss of postural tone and complete spontaneous recovery without medical intervention. This San Fran definition, however, is too non-specific , so I list more specific ECG abnormalities below: b. It is NOT a structured review or meta-analysis. Quinn et al.
The Case An 88-year-old woman with a history of dementia, major depressive disorder, and hyperlipidemia presented to the ED via EMS after a near syncopal episode. ECG approach to takotsubo syndrome: ECG cases: EM cases. She was weaned off of pressors and discharged four days after presentation to the ED with close cardiology follow up.
Written by Pendell Meyers, sent by anonymous, with additions by Smith A man in his 40s had acute chest pain and called EMS. EMS arrived and recorded this ECG: What do you think? Here is the PMcardio Queen of Hearts interpretation of the ECG: STEMI equivalent detected. Inferior and posterior OMI without STEMI criteria.
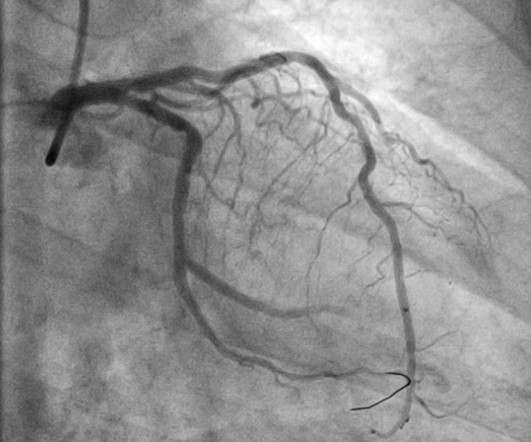
Despite the poor resolution of the 2 EMS ECGs the diagnosis of acute RCA OMI is immediately established by these EMS ECGs until proven otherwise. The Unmistakeable Conclusion: By the definition I suggested above today's patient manifests MINOCA. The cardiac cath was "normal".
This was written by one of our fine residents, who will soon be an EMS fellow: Michael Perlmutter Case A mid-50s male came to the ED with a burning sensation that was acutely worse while at home. This dynamic change is diagnostic of ACS. This was also non-diagnostic for OMI, although the dynamic changes are diagnostic of ACS.
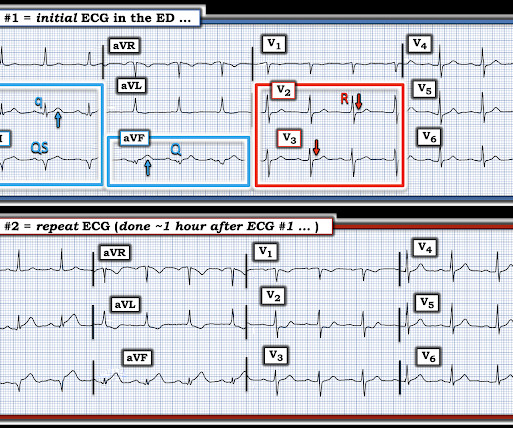
EMS arrived and recorded this ECG: What do you think? The ECG was transmitted to the Emergency Medicine physician who recognized inferior and posterior OMI findings, and confirmed that the patient has potential ACS symptoms. Figure-1: Comparison between the initial EMS ECG and the repeat ECG in the ED.
In the validation dataset, some cases lacked coronary angiography and relied on less definitive methods like CT or echo, adding variability and reducing the reliability of training and validation processes. Furthermore, the model was not trained on all comers in the emergency department, many of whom do not have ACS.
link] Differential Diagnosis Dermatologic manifestations Hypersensitivity reaction Food allergy Filariasis Ocular manifestations Loa loa infection Vitamin A deficiency Diagnosis The diagnosis of onchocerciasis typically requires tissue biopsy; thus, it is unlikely that the definitive diagnosis will be made in the emergency department.
link] Hummell AC, Cummings M. Cholera Case Definitions and Diagnosis.; Accessed October 5, 2024. link] Centers for Disease Control and Prevention (U.S.). History and Physical: Refugee Health Domestic Guidance.; Accessed October 5, 2024. Nutr Clin Pract Off Publ Am Soc Parenter Enter Nutr. 2022;37(1):41-49. doi:10.1002/ncp.10797
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content