This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Because the most severe LAD OMIs can cause ischemic failure of the RBB and LAF, any patient with ACS symptoms and new RBBB and LAFB with any concordant STE has LAD OMI until proven otherwise. There is no recognition of STEMI equivalency in this setting in the USA guidelines currently. Long term outcome is unavailable.
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. We documented that the majority of stenotic lesions had compensatory enlargement and thus exhibited remodeling. He does have a recently diagnosed PE, and has not been taking his anticoagulation due to cost. He was started on nitro gtt.
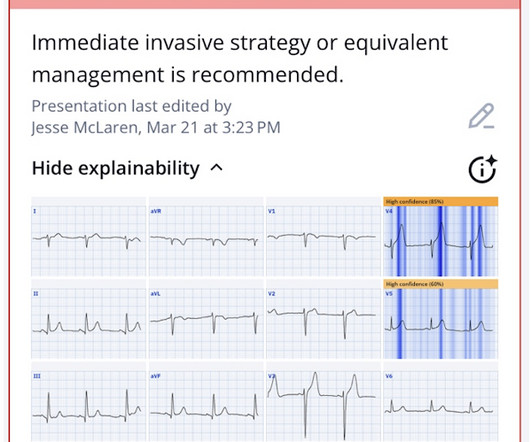
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. But there are also hyperacute T waves (HATW) in V4-5, which exclude early repolarization and pericarditis, leaving only LAD occlusion for this patient presenting with classic symptoms of ACS.
Based on recent studies, current guidelines recommend that O2 should not be given to non-hypoxemic patients with STEMI or NSTEMI [2,3]. REBEL Cast Ep114 – High Flow O2, Suspected ACS, and Mortality? 4159 patients (10% of total population) had STEMI 30d Mortality: High O2 protocol: 8.8% Low O2 protocol: 3.1%
Triage documented a complaint of left shoulder pain. Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Immediate versus delayed invasive intervention for non-stemi patients.
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). With EMS, patient had a GCS of 3 and was saturating 60% on room air. Both highly negative.
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS. Kosuge et al. Witting et al.
The Queen of Hearts agrees: Here the Queen explains why: However, it was not interpreted correctly by the providers: ED interpretation of ECG: "paced rhythm, LBBB but no STEMI pattern." Most large STEMI have peak troponin I in the 20.0 Next trop in AM. Peak trop 257.97 Smith: This is an enormous myocardial infarction. ng/mL - 80.0
Ongoing pain noted throughout all documentation, but after nitro drip and prn morphine, "pain improved to 2/10." Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Repeat ECG: New developing Q waves in V2 and V3, further confirming evolving OMI.
This patient could have very easily been overlooked, both because the ECG was STEMI negative and because the Q waves were attributed to an “old infarct”. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion. OMI or STEMI? As cardiology documented, “possible STEMI.
Furthermore, the term "STEMI equivalent" has no reliable or definable meaning except between two practitioners who both agree on the list of entities that they believe are STEMI equivalents and can agree on how to identify it. Obvious inferoposterior STEMI. J ACC 61(4):e78-140; page e83.
The documentation does not describe any additional details of the history. They also documented "Reproducible chest tenderness." Thus, these troponins are very concerning for ACS, and subsequent ones will probably be diagnostic of acute MI. The following ECG was obtained. ECG 1 What do you think? of the time.
He had no previously documented medical problems except polysubstance use. The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Is there STEMI? He reported a history of “Wolf-Parkinson-White” and “heart attack” but said neither had been treated. What is the rhythm? Moffat, M.
The AHA/ACC guidelines recommend emergent cardiac catheterization for patients with concern for ACS and refractory chest pain despite maximum medical therapy defined as aspirin + clopidogrel/ticagrelor + heparin/enoxaparin. link] He was admitted to the cardiology unit for serial troponin measurements and concern for possible ACS.
STEMI , ST-segment elevation acute myocardial infarction ). 1 Initial diagnosis of STEMI ECG Management Recommendation Level of evidence A 12-lead ECG should be interpreted immediately (within 10 minutes) at first medical contact. I C If possible, patients should bypass non-PCI centres to a PCI-capable centre.
These elevations meet STEMI criteria ( ≥ 1mm in 2 contiguous leads). While this may be change that is reciprocal to an Acute/Subacute Inferior STEMI, the problem is that LV aneurysm may also manifest with this reciprocal change. In STEMI, they are generally upright and large in proportion to the QRS. This case is tough.
He had no symptoms of ACS. The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS."
If it is maximal in V1-V4, and the patient's presentation in consistent with ACS (as this certainly is), then it is DIAGNOSTIC of Occlusion with 90% specificity (We have an upcoming article that proves this). Angiogram: "ACS - Non ST Elevation Myocardial Infarction. Because we are hypnotized the STEMI paradigm. "If
Prehospital ECG: Obvious anterolateral STEMI (Proximal LAD occlusion) The cath lab was activated prehospital by the medics. This is the longest lasting I have ever documented a hyperacute T wave without going "up" or "down." Interventionalist at the Receiving Hospital: "No STEMI, no cath. Here is one case of a patient I saw.
After rethinking the case, he remained concerned about ACS and subsequently performed a point-of-care ultrasound in order to evaluate for regional wall motion abnormality. We assume that at some point the patient's pain returned, but it is not documented, so exactly when this happened is uncertain. There is no age cut-off for ACS.
The triage ECG was interpreted correctly as "No STEMI." This finally prompted a repeat ECG at 1341: 1350: Obviously STEMI(+) OMI. Obvious ACS history with ongoing pain despite medical management and upgoing troponin is an indication for emergent cath regardless of ECG findings. = The second troponin returned higher at 45 ng/L.
This morphology can be cause by or associated with cocaine: A Patient with Cocaine Chest Pain and Prehospital Computer interpretation of STEMI This is OMI of the anterior, lateral, and inferior walls until proven otherwise. But it does not meet STEMI criteria and it was not initially recognized. ng/mL (very elevated).
He wrote in his note that "The EKG showed early repolarization in I, V2-V3 but no clear STEMI pattern." See far below for data on 24 troponin T in STEMI and NSTEMI, and correlation with infarct size. This difficulty results in high lateral OMI being the most commonly missed OMIs by the misguided STEMI criteria.
Authors state early cath may be of benefit in those with no STEMI, but much of the more recent literature suggests this is more controversial. Hematologic Management Takeaway : They recommend a transfusion threshold < 9 g/dL in those with ACS, but several studies (MINT trial) and guidelines suggest 8 g/dL can be used.
STEMI negative : the EMS automated interpretation read, “STEMI negative. According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists. Inferior infarct, age undetermined.
There is very scarce documentation, but the next ECG was obtained around 1 PM. Discussion: This case highlights many important points worthy of discussion, mainly because it represents very routine care for ACS but there are so many ways we could improve outcomes with tools we already have! There was no repeat ECG.
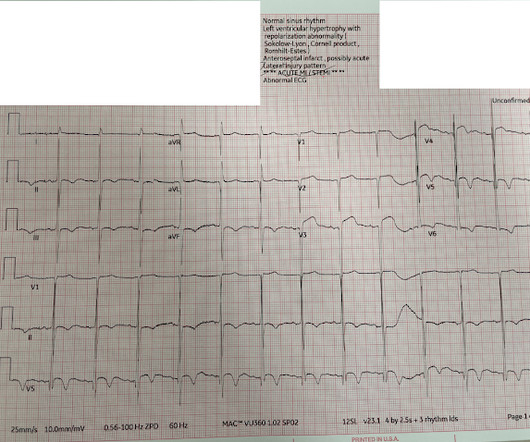
Even before we have clinical context, this ECG simply does not appear concerning for OMI, notwithstanding the machine's interpretation ** ** ACUTE MI / STEMI ** **. But in the world of STEMI, this is a challenging ECG to most. When the Queen has some suspicion of OMI, she asks if the patient has ACS Symptoms.
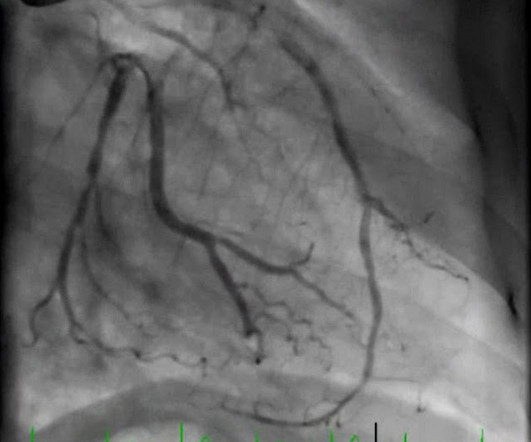
But thankfully, when the clinical context is clearly and highly concerning for ongoing ischemia from ACS, this distinction doesn't matter much. The note documents that the first view of the LCX showed 99%, TIMI 2 flow, but then (before intervention) was seen to fully occlude in real time (100%, TIMI 0).
After completing the ACS algorithm with amiodarone and lidocaine, there are diminishing returns on further treatments. International expert consensus document on takotsubo syndrome (part I): Clinical characteristics, diagnostic criteria, and pathophysiology. Or was it out of proportion, perhaps worsened by the sympathetic surge?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content