This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The 2022 American College of Cardiology (ACC) pathway provides timely guidance [1]. Encourage your ED to set up an algorithm that you can follow based on your laboratory’s assay. Low-risk patients do not routinely require stress testing in the ED. We help you translate this to your clinical practice, by illustrating with a case.
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. C Examination notable for diaphoresis, 1+ bilateral lower extremity edema, regular heart rate and rhythm, and no signs of respiratory distress with normal breath sounds. looked at consecutive patients with PE, ACS, or neither.
Today on the emDOCs cast with Brit Long, MD ( @long_brit) , we cover acute chest syndrome part 1. Episode 100: Acute Chest Syndrome Part 1 Background SCD is an autosomal recessive condition that results in the formation of hemoglobin S (HbS). Each episode of ACS has a 9% mortality rate. pneumoniae, C. pneumoniae, C.
The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. Moreover , the patient has ongoing symptoms and has an unexplained elevated troponin, so she is having an MI and the only question is whether it is type 1 or type 2 due to hypertension. At midnight.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chest pain onset around 9 PM the evening prior. ECG 1 What do you think? Grines, C.
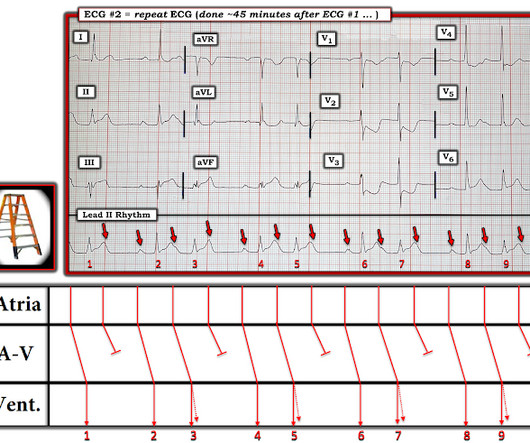
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. Challenge QUESTION: The relative change in T-QRS-D is not the only thing that changes during period of time that passed between recording of the 2 ECGs shown in Figure-1.
Sickling leads to vascular occlusion, end-organ ischemia, and decreased RBC lifespan, which, in turn, leads to pain crisis, acute anemia, sequestration, infection, and acute chest syndrome (ACS). ACS is lung injury due to vaso-occlusion in the pulmonary vasculature; many with ACS will have a concomitant vaso-occlusive pain crisis.
2024 Oct 9. There were no differences in survival (12% with IO vs 10% with IV) or neurologically intact survival (9% vs 8%). 2024 Nov 1. Restrictive vs Liberal Transfusion Strategy in Patients With Acute Brain Injury: The TRAIN Randomized Clinical Trial. doi: 10.1001/jama.2024.20424. 2024.20424. Shorter courses of antibiotics.
He has already climbed Ben Nevis in Scotland, visited the Gobi desert (possibly from the comfort of his parents 4 x 4, but who’s judging) and has his bronze D of E nailed. All you know, back in ED, is that the ETA is 10 minutes, and there is a single stab wound to the chest. A PEM Adventure Ranulf is a 14-year-old explorer.
[link] Case continued She arrived in the ED and here is the first ED ECG. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. IMPRESSION: 1. The Queen no longer thinks it is OMI.
Here is the first ED ECG recorded, now pain free after sublingual Nitro: There is what appears to be a reperfusion T-wave in I and aVL. Learning Point: 1. For examples of such exceptions — See My Comment in the January 9, 2019 — August 22, 2020 — and June 30, 2023 posts in Dr. Smith's ECG Blog ).
Episode 108: Unexplained Sinus Tachycardia Mental Model Background: When a patient in the ED has sinus tachycardia our job as emergency physicians is to identify and treat of the underlying pathology. Discharging a patient with abnormal vital signs has been linked to unanticipated death (1-4). 2005;2(1):44-52. Clin Cardiol.
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Despite not being considered in this category, opioid medications are sometimes given for ACS. Am Heart J.
Sent by anonymous, written by Pendell Meyers A man in his late 40s presented to the ED with concern for allergic reaction after accidentally eating a potential allergen, then developing an itchy full body rash and diarrhea. In the ED he received methylprednisolone, diphenhydramine, and epinephrine for possible anaphylaxis.
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chest pain. On review of systems the patient reported back pain for approximately 1 week which he was treating with NSAIDs with minimal relief. 15-9/6/2017 ). His first troponin T then resulted elevated at 0.19
1 The American College of Surgeons’ (ACS) Trauma Quality Improvement Program (TQIP) Massive Transfusion in Trauma Guidelines leave a good amount of flexibility for hospitals regarding transfusion protocols, focusing more on systems-level aspects of designing and implementing MTPs.2,3 in the 1:1:1 group vs. 17.0%
mm in just one lead V7-9), but as far as I can tell all of these documents specifically avoid calling this condition STEMI and specifically avoid using any terminology similar to "STEMI equivalent." I focus My Comments on 3 of the ECGs that were shown in this case ( Figure-1 ). This was interpreted as "no significant change."
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. mm of ST segment elevation, V2 and V3 have 1 mm of elevation, v4 has 2 mm of elevation and v5 around 1.5 Learning Points: 1. What do you think? V1 has 0.5
One of the most hair-raising presentations to the emergency department (ED) can be massive hemoptysis with respiratory failure. or 9 size endotracheal tube to allow for bronchoscopy and/or endobronchial blocker placement whenever necessary. These patients are at imminent risk of respiratory failure. A special thanks to Drs.
This is a 30-something healthy patient presented with COVID pneumonia who presented to the ED. Here they are: Learning Points: 1. Type 1 and 2 Myocardial Infarction and Myocardial Injury: Clinical Transition to High-Sensitivity Cardiac Troponin I. Am J Med [Internet] 2017;130(12):1431–9.e4. He was moderately hypoxic.
The ED physician read this as "Normal sinus rhythm. Obvious STEMI(+) OMI of inferior, posterior, and lateral walls, now with likely 2nd degree heart block type 1 (Wenckebach). STD maximal in V1-V4, without a QRS abnormality causing it, and in the setting of ACS symptoms, is posterior OMI until proven otherwise. Easy for anyone.
There are two main etiologies of ischemic ST-depression: 1) subendocardial ischemia 2) reciprocal to ST-elevation in an opposite wall Here there are distinct R-waves with marked ST-depression throughout most of the precordium. Tips for recognizing Acute Posterior STEMI: 1. References: 1. This can help in confirmation.
Due in large part to the proliferation of anonymous chemical factories able to produce industrial volumes of inexpensive synthetic opioids without opium or other controlled precursors, fentanyl spilled into the United States, Canada, and Europe, heroin soon fell to market forces [1, 2]. Some patients require re-dosing in the ED.
As the only respiratory therapist in the ED has been paged and is starting BiPAP for this patient, an overhead call for two incoming trauma alerts from a multivehicle collision sounds. Importantly, the comparison between an ABG and VBG is site-specific, as illustrated below (Table 1) (1, 3-6).
Pre-school wheezers remain a poorly understood cohort of children despite seeing them every day in paediatric EDs. However, there was no difference in LOS (83 minutes for placebo vs 79 minutes for prednisolone) in participants who were discharged straight from the ED ( 32% ). study from 200 9. What does it mean to our patients?
A 64-year-old male presents by EMS to the ED with shortness of breath. 1 There are over 50,000 visits related to heart transplant in the United States each year and over half of these patients are admitted to the hospital from the ED. We’ll keep it short, while you keep that EM brain sharp.
1 His description of cases of life-threatening infections in the perineal, genital or perianal regions were thought to be idiopathic in previously healthy men. 3-5 Fournier gangrene is a type of necrotizing soft tissue infection, which can be categorized into four types based on the infectious organism involved and other features (Table 1).
A 67-year-old man presents to the emergency department (ED) in cardiac arrest. On ED presentation, he is unresponsive and the monitor shows ventricular fibrillation. 2018;13(9):e0204169. Margey R, Browne L, Murphy E, et al. Emmerson AC, Whitbread M, Fothergill RT. Cortez E, Krebs W, Davis J, et al.
An 8-year old male with a history of sickle cell anemia presents to the ED for evaluation of fever for 2 days and “feeling like I can’t get a full breath”. 2 mcg/kg, max 100 mcg) while obtaining IV access 20 IV/IM ketorolac (1 mg/kg, max 15 mg) Morphine (05-0.1 C or 100.4 mg/kg, max 4 mg per dose q20-30min) or hydromorphone (0.01-0.02
Jafar Mahmood, MD (Pain Medicine Attending, Paincare Medical Practice) // Reviewed by: Jessica Pelletier, DO, MHPE (EM Attending, APD, University of Missouri-Columbia), Marina Boushra, MD (EM-CCM Attending, Cleveland Clinic); Brit Long, MD (@long_brit) Introduction: Pain management in the ED can be a unique challenge.
F, HR 48, RR 28, BP 104/62, SPO2 88% on non-rebreather mask The patient’s friend who brought her to the ED tells you the patient made suicidal statements earlier in the day and was found in her yard shed. 1-5 Farmers also treat sheep for parasites using OPs and may become symptomatic after exposure, an illness called Dipper’s Flu.
Patellar reflexes are 1+. 1, 2, 4, 9 Organophosphates are one of many types of insecticide and are used worldwide to manage crops. 1, 2 Symmetric sensorimotor axonopathy: leg cramping to extremity weakness and paralysis. 1, 2 Sensory > Motor neurons with predilection for long axons. Muscle tone is normal.
She describes the pain as left-sided, non-radiating, and 9/10 in severity. Answer: Takotsubo Cardiomyopathy 1-18 Background: Also known as transient apical ballooning syndrome, apical ballooning cardiomyopathy, stress-induced cardiomyopathy, stress cardiomyopathy, Gebrochenes-Herz syndrome, and broken-heart syndrome.
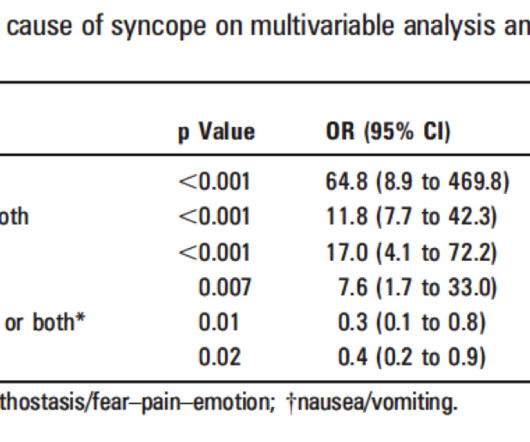
Summary of ED Approach to Syncope Please excuse the formatting problems, which I have not been able to fix! Cardiac Syncope ("True Syncope") Independent Predictors of Adverse Outcomes condensed from multiple studies 1. Palpitations preceding syncope (highest value on EGSYS score) 9. Abnormal ECG – looks for cardiac syncope.
Figure 1: Clinical manifestations and long-term consequences of sickle cell disease Training and education on sickle cell disease: Training and education are crucial to improve morbidity and mortality. with thanks A 15-month-old Kenyan boy presents to ED with right hand swelling. Blood culture is pending.
She arrived to the ED with a nonrebreather mask. The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. The ED physician noted Once her respiratory status improved, her EKG looks much improved with no evidence of STEMI. Management?
In contrast to traditional teams that have the luxury of time for their members to build rapport, teams in the emergency department (ED) change every day. 1,2 As Edmondson described, ED teams disband almost as quickly as they are assembled. Harvard professor Amy C. 4 Can AI Help with Teaming? 4 Can AI Help with Teaming?
Using data from the Danish Fetal Medicine Database (from 2008 to 2018), it found that pregnancies with MCHDs had a significantly higher rate of complications such as preeclampsia, preterm birth, and foetal growth restriction compared to those without MCHDs (23% versus 9%), except for transposition of the great arteries. 2024 Dec 21;184(1):98.
1 Life Cycle and Pathophysiology Life Cycle Humans are the only hosts for O. 1 The parasite has a 5-stage life cycle in which the blackfly acts as an obligate intermediate host. The worms can live as long as 15 years, and female worms may produce microfilariae (early-stage larvae) for up to 9 of those years. 13 Figure 1.
ED Evaluation Transport to the ED from the refugee reception center takes 1 hour. Labs Laboratory workup in the ED is notable for a leukocytosis of 41,000/L, hemoglobin of 6.5 g/dL, thrombocytopenia of 96 10 9 /L, prothrombin time (PT) of 16.1 1 By the end of 2023, 117.3 of the global population.
The syphilis and trichomonas tests come back negative in the ED, but his rapid HIV test is positive. How should clinicians approach the diagnosis and management of HIV in the ED? 9 Historically, the management of HIV and its complications was primarily the domain of primary care and infectious disease (ID) specialists.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content