This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
At the time of ED arrival he was alert, oriented, and verbalizing only a headache with a normalized BP. The ED activated trauma services, and a 12 Lead ECG was captured. This was deemed “non-specific” by the ED physicians. Thus, the ED admission ECG changes cannot be blamed on LVH. The fall was not a mechanical etiology.
In the age of high sensitivity troponins and the HEART pathway, which patients are safe to discharge home from the ED? What are the most useful historical factors to increase and decrease your pretest probability for ACS? Which cardiac risk factors have predictive value for ACS?
Trauma season is at hand and like all other pediatric emergency departments in the country, we find our ED breaking ( pun intended ) at the seams with orthopedic injuries. We see all different flavors of upper extremity injuries. The minority of parents would have wanted clinic follow up (6%) and reimaging (14%). J Bone Joint Surg Br.
Our experience: Traditionally, ED physicians do not like ordering urine drug screens (UDS). In our study, we used COWS alone in the ED, which does utilize restlessness, anxiety, and tachycardia as part of the formula, as the sole evaluation tool for tranq dope withdrawal. Some patients require re-dosing in the ED. 2023 [book].
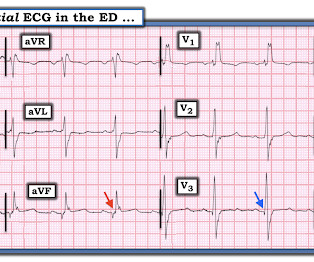
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
European Journal of Internal Medicine , [link] You can listen to my 27-minute rant on Youtube here: [link] This multinational trial looked at a three-pronged diagnostic protocol in the ED for adults with suspected acute aortic syndromes. The protocol used the ADD score, a POCUS echo protocol and D-dimer to try and exclude AAS in the ED.
You turn to the attending and ask, “do you really think this could be acute coronary syndrome (ACS)?” ACS is usually amongst this differential, as cardiovascular disease is a leading cause of morbidity and mortality in this population. The proportion of patients with ACS at the index visit or within 30 days. *
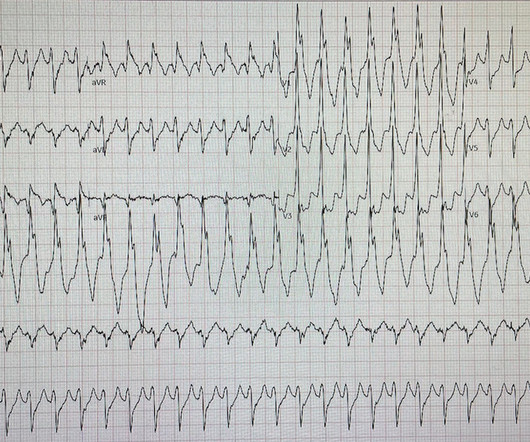
David Didlake EMT-P, RN, ACNP @DidlakeDW An adult male self-presented to the ED with palpitations and the following ECG. I interpreted the ECG as VT with two primary etiological possibilities: 1. Abrupt plaque ulceration of Type 1 ACS leading to VT. The patient was very uncomfortable, dyspneic, and displayed an SpO2 90% on RA.
However, many institutions’ surgical teams still require or request a formal study over a bedside exam, likely due to a lack of confidence in the accuracy of POCUS, resulting in longer ED stays. ACS surgeons appeared to select surgery as their initial choice substantially more frequently than other subspecialties.
A 5-year-old female presented to the emergency department (ED) with a one-year history of gradually increasing anterior neck swelling. She was discharged from the ED on levothyroxine 25 mcg daily with endocrinology outpatient follow-up. The patient had no significant past medical history. Pediatric neck masses. Pediatr Rev.
They also discuss the challenges of pulse palpation and the need for more rigorous research in EMS and ED settings. References: Kimbrell J, Kreinbrook J, Poke D, Kalosza B, Geldner J, Shekhar AC, Miele A, Bouthillet T, Vega J. They emphasize the importance of confirming electrical capture before assuming mechanical capture.
Although the attending crews did not consider the ECG pathognomonic for occlusive thrombosis, they nonetheless considered the patient high-risk for ACS and implored him to reconsider. Here is the final ECG just prior to ED transfer. It’s important to stress the presence of a normal QRS (i.e., The pathology is now painfully evident.
The patient was brought to the ED and had this ECG recorded: What do you think? Then assume there is ACS. After 1 mg of epinephrine they achieved ROSC. Total prehospital meds were epinephrine 1 mg x 3, amiodarone 300 mg and 100 mL of 8.4% sodium bicarbonate. And what do you want to do?
Case: You are working a shift in your local community emergency department (ED) when a 47-year-old male presents with chest pain. Background: Chest pain is one of the most common presentations to the ED. In prior decades nearly all patients presenting to EDs with chest pain were admitted to hospital. AEM June 2022.
Case: A 46-year-old female presents to the emergency department (ED) with sudden onset, severe right flank pain. Delays in providing adequate analgesia leads to poorer patient outcomes, prolonged ED length of stay and reduced patient satisfaction (17, 18). AEM Feb 2021. Reference: Brichko et al.
He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP). She arrives in the emergency department (ED) with decreased level of consciousness and shock.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). ACS and hyperkalemia both have lethal downstream consequences, so it is imperative for the clinician to acclimate to the presentation, or developing, features of each. ECG's are difficult. Hyperkalemia revisited.
The person I was texting knows implicitly based on our experience together that I mean "Definite posterior OMI, assuming the patient's clinical presentation is consistent with ACS." The interventional cardiologist then canceled the activation and returned the patient to the ED without doing an angiogram ("Not a STEMI").
David Didlake, FF/EMT-P, AG-ACNP @DidlakeDW An elder female presented to the ED with worsening shortness of breath. This should prompt immediate investigation into supply-demand mismatching, or ACS. She was known to have a history of poorly controlled COPD, AFib, and multivessel coronary disease.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? The ST depressions in I and aVL have resolved.
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (ret) @DidlakeDW Expert commentary and peer review by Dr. Steve Smith [link] @smithECGBlog A 57 y/o Female with PMHx HTN, HLD, DM, and current use of tobacco products, presented to the ED with chest discomfort. A 12 Lead ECG was captured on her arrival.
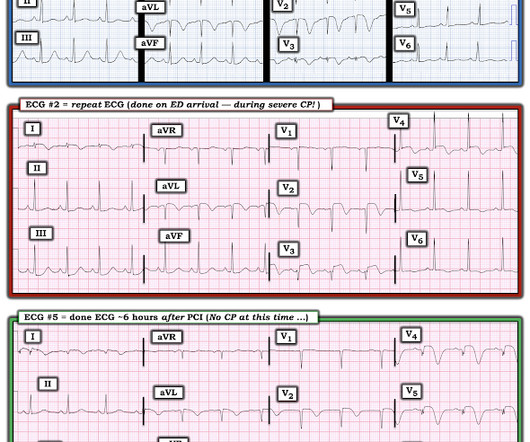
This is acute ACS, but it almost always seen in a pain free state. An ED ECG, if recorded with pain, should show LAD OMI. That said — severe chest pain was present at the time the patient arrived in the ED ( corresponding to the time ECG #2 was recorded ).
[link] Case continued She arrived in the ED and here is the first ED ECG. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. I don't know if her pain was getting better or not.
AEM May 2022 Guest Skeptic: Dr. Justin Morgenstern is an emergency physician and the creator of the #FOAMed project called First10EM.com Case: A 33-year-old male presents to the emergency department (ED) complaining of abdominal pain. He doesn’t have any specific symptoms today, including no fever, vomiting, diarrhea, or urinary symptoms.
He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines. Here is the initial ED ECG. What do you think? Rhythm : Residents asked me why it is not VT. The QRS is extremely wide.
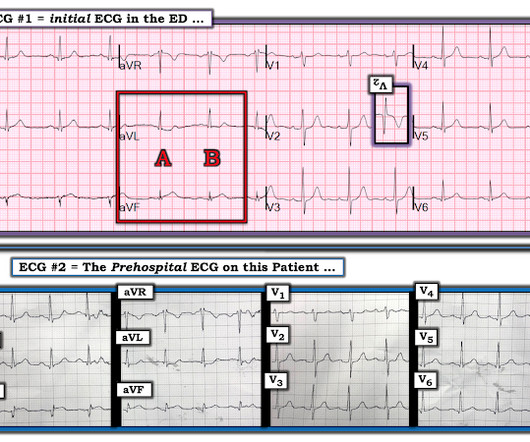
Jerry Jones commented: "Any ST depression on the ECG of a patient with chest pain credible for ACS represents a reciprocal change until proved otherwise." For clarity — I show in Figure-1 the i nitial E CG obtained in the ED ( = E CG # 1 ) — together with the p rehospital E CG that I have pieced together ( = E CG # 2 ).
There were zero patients in this study with a "normal" ECG who had any kind of ACS! Figure-1: I've labeled the initial ECG in the ED. KEY Point: All patients who present to the ED for new CP should promptly have a triage ECG recorded, that is then immediately interpreted by the ED physician.
Cardiology consult note written around that time documents that "Pain improved with NTG, morphine in ED but still present." As a result, even before looking at this patient's initial ECG — he falls into a high -prevalence likelihood group for ACS ( for an A cute C oronary S yndrome ). Repeat cTnI drawn at around 8 AM was 3.910 ng/mL.
A middle-aged man complained of 15 minutes of classic angina that resolved upon arrival to the ED. But it does prove that the patient has coronary disease and makes the probability that his chest pain is due to ACS very very high. Figure-1: The initial ECG that was done in the ED ( See text ).
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Link to abstract Link to full text 2) Use of Morphine in Non-STE-ACS is independently associated with mortality, at odds ratio of 1.4
Here was his initial ED ECG: There is atrial fibrillation with a rapid ventricular response. Does this patient have ACS? He did not have ACS. The remainder were due to other etiologies, (including NonSTEMI ACS). But approximately 50% were due to non-ACS etiologies. A middle-aged male had a V Fib arrest.
Prior episodes had simply resolved after brief symptoms, but the current episode had lasted for 2 hours without improvement, so she presented to the ED. At triage she stated her pain is still persistent, but it is mildly improved compared to when she decided to come to the ED. No diaphoresis or vomiting.
Written by Jesse McLaren A 75 year-old patient with diabetes and end stage renal disease was sent to the ED after dialysis for three days of nausea, vomiting, loose stool, lightheadedness and fatigue. But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. Below is the 15 lead ECG.
His parent noticed a dental problem and immediately brought the patient to the ED. The patient was walking his dog when it ran after a squirrel. The patient was pulled forward, causing him to hit his tooth on the asphalt. The physical exam is shown below. Which of the following is the best next recommendation? Dent Traumatol.
The Queen of Hearts agrees: Here the Queen explains why: However, it was not interpreted correctly by the providers: ED interpretation of ECG: "paced rhythm, LBBB but no STEMI pattern." The cath report showed: Significant stenosis with subtotal occlusion (99%) in the prox to mid Lcx, culprit of ACS, TIMI flow 1.
Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Cardioversion will address the rhythm problem immediately, also if the chest discomfort subsides when SR is restored, ischemia from ACS becomes much less likely. This patient presented to the ED “after a couple of days of chest discomfort”.
Here is the first ED ECG recorded, now pain free after sublingual Nitro: There is what appears to be a reperfusion T-wave in I and aVL. The 3rd tracing in Figure-1 was the initial ED ECG — obtained at a time when the patient's CP had resolved. Shortly thereafter, on arrival in the ED — ECG #3 was recorded.
The machine indicated STEMI (but it barely meets STEMI criteria, if at all) and the patient was brought to the ED: On arrival 20 minutes later the pain had reduced to 1/10 after aspirin, and the patient had repeat ECG at triage: Now the ST segments and T waves have normalized, and the only abnormality is sinus bradycardia and loss of R waves.
mL/kg/hr for 2 consecutive hours OR Decrease in serum lactate by more than 10% from initial level Primary outcome – Early norepinephrine group vs. the control group demonstrated higher rates of shock control at 6 hours: 76.1% vs 48.4% (OR 3.4, vs 48.4% (OR 3.4,
I delved into his reasons for arriving so late after onset, thinking that perhaps the pain had only recently increased, or that it had been intermittent until now, but he confirmed that it was 14 hours of constant pain and it was his significant other who insisted that he go to the ED. Patients with ACS and hemodynamic instability 2.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. In our opinion it should not be given in ACS unless you are committed to the cath lab.
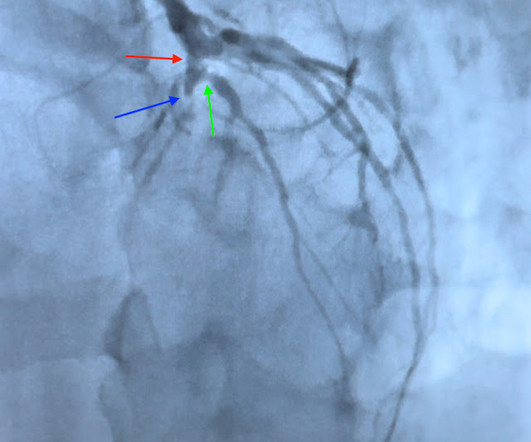
He sent the patient to the ED for further evaluation. A chest x-ray in the ED found bilateral pleural effusions. The patient was admitted from the ED and finally had an angiogram the next morning: Angiogram : Image 1: This is the LAO caudal, or spider projection. There are hardly any R waves in any of the precordial leads!
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Around 19 hours later, he experienced the same pain, which prompted his presentation to the ED.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content