This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Bupe Allergy Buprenorphine induction has been the mainstay of emergencydepartment treatment of opioid use disorder for more than a decade [11, 12]. Our experience: Traditionally, ED physicians do not like ordering urine drug screens (UDS). Some patients require re-dosing in the ED. 2023 Aug 1;89(2):231. 2023 [book].
Trauma season is at hand and like all other pediatric emergencydepartments in the country, we find our ED breaking ( pun intended ) at the seams with orthopedic injuries. Pediatr Emerg Care. We see all different flavors of upper extremity injuries. J Bone Joint Surg Br. 2001;83:1173-5. Oakley EA, Ooi KS, Barnett PLJ.
You turn to the attending and ask, “do you really think this could be acute coronary syndrome (ACS)?” Background: Patients 65 years and older account for about 15% of emergencydepartment visits in the United States. The proportion of patients with ACS at the index visit or within 30 days. * Reference: Wang et al.
Rapid Administration of Methoxyflurane to Patients in the EmergencyDepartment (RAMPED): A Randomised controlled trial of Methoxyflurane vs Standard care. […] The post SGEM#320: The RAMPED Trial – It’s a Gas, Gas, Gas first appeared on The Skeptics Guide to Emergency Medicine. Reference: Brichko et al. Reference: Brichko et al.
A 5-year-old female presented to the emergencydepartment (ED) with a one-year history of gradually increasing anterior neck swelling. She was discharged from the ED on levothyroxine 25 mcg daily with endocrinology outpatient follow-up. The patient had no significant past medical history. Pediatric neck masses.
1 It is a quickly deployable and easily interpreted study that can be done in real time to guide decisions in the EmergencyDepartment. However, many institutions’ surgical teams still require or request a formal study over a bedside exam, likely due to a lack of confidence in the accuracy of POCUS, resulting in longer ED stays.
Corey Heitz is an emergency physician in Roanoke, Virginia. He is also the CME editor for Academic Emergency Medicine. Corey Heitz is an emergency physician in Roanoke, Virginia. He is also the CME editor for Academic Emergency Medicine. Background: Chest pain is one of the most common presentations to the ED.
Guidelines for Reasonable and Appropriate Care in the EmergencyDepartment (GRACE) 2: Low-Risk, Recurrent Abdominal Pain in the EmergencyDepartment. Guidelines for Reasonable and Appropriate Care in the EmergencyDepartment (GRACE) 2: Low-Risk, Recurrent Abdominal Pain in the EmergencyDepartment.
Kaushal Khambhati is also a fourth-year resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. She arrives in the emergencydepartment (ED) with decreased level of consciousness and shock. She has a history of hypertension and non-insulin dependent diabetes mellitus.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). ACS and hyperkalemia both have lethal downstream consequences, so it is imperative for the clinician to acclimate to the presentation, or developing, features of each. ECG's are difficult. link] [1] Zachary et al.
It is commonly used in EmergencyDepartments, especially in febrile and possibly infectious patients. ACS and Aortic Dissection - For ACS and Dissection, the higher CRP levels, the worse prognosis. It is not used to diagnose ACS/Dissection. Utility of CRP 1. Like other biomarkers, it does not stand alone.
Background Information: Atrial fibrillation with rapid ventricular rate (RVR) is one of the many tachydysrhythmias we encounter in the EmergencyDepartment (ED). Amiodarone versus digoxin for acute rate control of atrial fibrillation in the emergencydepartment. Am J Emerg Med. Paper: Mason JM, et al.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? The ST depressions in I and aVL have resolved.
, tells us that we physicians do not need to even look at this ECG until the patient is placed in a room because the computer says it is normal: Validity of Computer-interpreted “Normal” and “Otherwise Normal” ECG in EmergencyDepartment Triage Patients I reviewed this article for a different journal and recommended rejection and it was rejected.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. Upon arrival to the emergencydepartment, a senior emergency physician looked at the ECG and said "Nothing too exciting." References: 1.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergencydepartment at around 3 AM complaining of chest pain onset around 9 PM the evening prior.
A man in his 90s with a history of HTN, CKD, COPD, and OSA presented to the emergencydepartment after being found unresponsive at home. Vital signs were within normal limits on arrival to the EmergencyDepartment. EKG on arrival to the ED is shown below: What do you think? Blood glucose was not low at 162 mg/dL.
A 35-year-old male presented to the emergencydepartment complaining of chest pain that started 1.5 FIGURE 1: First ED EKG. FIGURE 2: Baseline ED from 2 months prior. FIGURE 3: Second ED EKG. Dr. Young is an emergency physician at Saint Francis Hospital and Medical Center, Hartford, Conn. Click to enlarge.)
She presented to the emergencydepartment after a couple of days of chest discomfort. Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? This patient presented to the ED “after a couple of days of chest discomfort”. The last echocardiography 12 months ago showed HFmrEF.
Arch Dis Child Fetal Neonatal Ed. Arch Dis Child Fetal Neonatal Ed. Invasive bacterial infection in children with fever and petechial rash in the emergencydepartment: a national prospective observational study. De Alwis AC, et al. Eur J Pediatr. 2023 Apr 21. Kuypers KLAM, et al. Hegeman EM, et al. 2023 Apr 18.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Around 19 hours later, he experienced the same pain, which prompted his presentation to the ED.
Smith: If this is ACS (a big if), t his is just the time when one should NOT use "upstream" dual anti-platelet therapy ("upstream" means in the ED before angiography). History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Anything more on history?
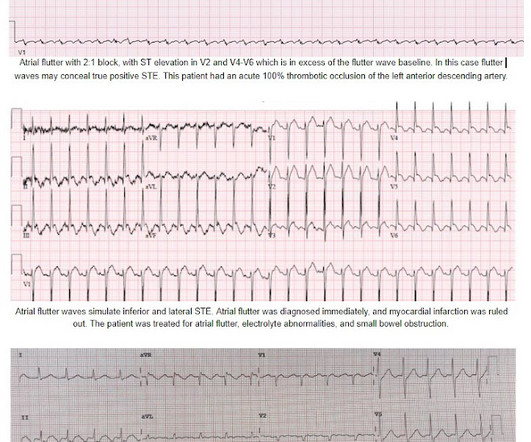
An ECG was recorded quickly on return to the ED: (sorry for poor quality, cannot get originals) What do you think? On arrival to the PCI center's EmergencyDepartment, the receiving team recorded an ECG on arrival: Persistent atrial flutter, however this time the QRS occurs on a slightly different portion of the flutter wave.
I finished my residency of Emergency Medicine and I’m working at a great EmergencyDepartment here in Brazil. Case "Male, 43yo, come to ED with Epigastric Pain started 3 hours ago. Since then, I started looking for OMI EKG findings and not just STEMI. Risk Factors: High Cholesterol.
The NIHSS cutoff that predicts outcomes is 4 points higher in AC compared with PC infarctions. Median time from ED arrival to diagnosis was 8 hours 24 min in one study, with only 19% being diagnosed within the 4.5-hour Post TW, ed. NIHSS does have limitations when applied to posterior circulation (PC) strokes. Neurohospitalist.
A 67-year-old man presents to the emergencydepartment (ED) in cardiac arrest. On ED presentation, he is unresponsive and the monitor shows ventricular fibrillation. Canadian Journal of Emergency Medicine. Emmerson AC, Whitbread M, Fothergill RT. 20(S1):S67. Resuscitation. 2017;117:97-101.
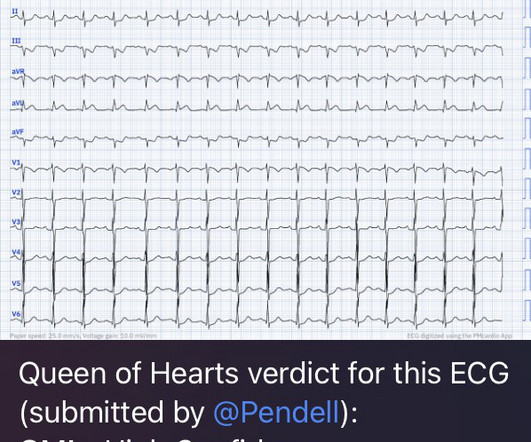
One case sent by Dr. Sean Rees MD, written by Pendell Meyers, other case by Sam Ghali and Steve Smith Take a look at these two ECGs below from two patients in the ED, first without any clinical context. He had no symptoms of ACS. The remainder of his EmergencyDepartment stay was uneventful. QOH: "OMI High confidence".
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergencydepartment with substernal chest pain for 3 hours prior to arrival. The screening physician ordered an EKG and noted his ashen appearance and moderate distress. Triage EKG: What do you think?
52-year-old lady presents to the EmergencyDepartment with 2 hours of chest pain, palpitations & SOB. Most, but not all, ECG “aneurysm morphology” is associated with an actual aneurysm on Echo ( see this case with ED bedside echo ). Beware of ACS presenting with atypical symptoms, including absence of chest pain.
Encourage your ED to set up an algorithm that you can follow based on your laboratory’s assay. Low-risk patients do not routinely require stress testing in the ED. You (or someone in your department) needs to know which assay your ED has, and use the appropriate values for that assay.
She was brought to the EmergencyDepartment and this ECG was recorded while she was still feeling nauseous but denied chest pain, shortness of breath, or other symptoms: What do you think? I wouldn't activate the lab for this EKG alone, but if the patient is clinically compatible with ACS you could call a heart alert.
This is the initial ED ECG of a 46 year old male with chest pain: The QTc was 420 ST Elevation at 60 ms after the J-point in lead V3 = 2.5 consistent with LAD occlusion) This prompted serial ECGs: These dynamic changes confirmed ACS There was a large obtuse marginal 100% occlusion (surprisingly not LAD! 100% LAD occlusion.
Case: You are working a busy shift in a rural emergencydepartment (ED) and your excellent Family Medicine trainee presents a case of a 63-year-old woman with chest pain and some intermittent radiation into the inter-scapular region. The patient has no specific risk factors for acute coronary syndrome (ACS) or dissection.
However, RSI has never been shown to reduce the risk of aspiration in the ED (13) or during emergent OR cases (14). While RSI should remain the gold standard in the vast majority of patients in the ED, FI presents an additional technique to mitigate anatomic or physiologic risk. We don’t want to go backwards!
The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). The patient was rushed to the nearest emergencydepartment (non-PCI facility) for stabilization.
The patient is an adult male with a gunshot wound to the chest, and they’re combative with emergency medical services (EMS). According to a recent study in the Journal of Surgical Research [3] , 44% of all penetrating thoracic trauma patients presented to a non-trauma center (not a level 1 or level 2 ACS defined trauma center).
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the EmergencyDepartment via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. looked at consecutive patients with PE, ACS, or neither. What do you think? ng/mL, BNP 2790, and lactate 3.7.
Case submitted and written by Dr. Mazen El-Baba and Dr. Emily Austin, with edits from Jesse McLaren A 50 year-old patient presented to the EmergencyDepartment with sudden onset chest pain that began 14-hours ago. The pain improved (6/10) but is persisting, which prompted him to visit the EmergencyDepartment. Shroff, G.
Pre-school wheezers remain a poorly understood cohort of children despite seeing them every day in paediatric EDs. However, there was no difference in LOS (83 minutes for placebo vs 79 minutes for prednisolone) in participants who were discharged straight from the ED ( 32% ). Reattendance to GP/ED was more important.
The sensitivity of these scores range, but they cannot exclude FG diagnosis and may have lower sensitivity when used for prediction in ED patient populations. Wysoki MG, Santora TA, Shah RM, Friedman AC. West J Emerg Med. West J Emerg Med. fold increased odds of mortality, respectively. Fournier gangrene.
The ECG’s were sent to the PCI center, and the providers in the respective ED identified the T wave characteristics mentioned above. Such aggressive investigation was particularly warranted in this case because of symptoms compatible with ACS, as well as an equally frightening revelation of family history. link] [1] Mirand, D.
Notoriously elusive, with a high misdiagnosis rate, thoracic aortic dissection (AD) can mimic many conditions, including acute coronary syndrome (ACS, the most common), gastroesophageal reflux disease (GERD), stroke, and spinal-cord compression. The patient is admitted for ACS to a cardiologist who says he will see the patient in the morning.
Episode 108: Unexplained Sinus Tachycardia Mental Model Background: When a patient in the ED has sinus tachycardia our job as emergency physicians is to identify and treat of the underlying pathology. Lactate Troponin Could this be ACS or myocarditis? In the ED, our job is to identify and treat underlying causes.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content