This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
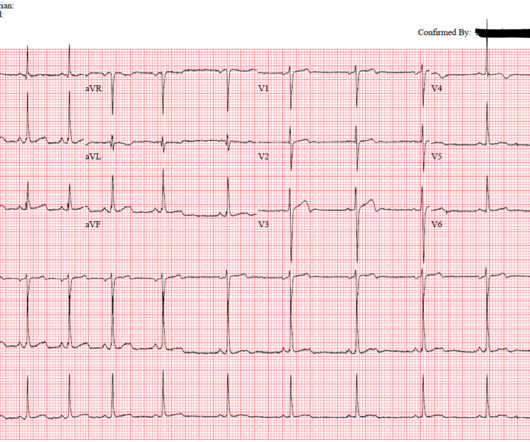
David Didlake @DidlakeDW EMS personnel responded to the residence of an 81 y/o Male with syncope. At the time of ED arrival he was alert, oriented, and verbalizing only a headache with a normalized BP. The ED activated trauma services, and a 12 Lead ECG was captured. This was deemed “non-specific” by the ED physicians.
Trauma season is at hand and like all other pediatric emergency departments in the country, we find our ED breaking ( pun intended ) at the seams with orthopedic injuries. The post Rebaked Morsel: Pediatric Buckle and Greenstick Forearm Fractures appeared first on Pediatric EM Morsels. J Bone Joint Surg Br. 2001;83:1173-5. Pediatrics.
Case A patient arrives via EMS from the bus station complaining of fever, vomiting, and back pain. Our experience: It was not long ago that we instructed our staff that: ‘COWS >8, give ’em 8 (mg of buprenorphine).’ Our experience: Traditionally, ED physicians do not like ordering urine drug screens (UDS). 2023 [book].
In the age of high sensitivity troponins and the HEART pathway, which patients are safe to discharge home from the ED? What are the most useful historical factors to increase and decrease your pretest probability for ACS? Which cardiac risk factors have predictive value for ACS?
They also discuss the challenges of pulse palpation and the need for more rigorous research in EMS and ED settings. References: Kimbrell J, Kreinbrook J, Poke D, Kalosza B, Geldner J, Shekhar AC, Miele A, Bouthillet T, Vega J. They emphasize the importance of confirming electrical capture before assuming mechanical capture.
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. Type 2 MI is common in the ED and can result from vigorous exercise (common in athletes after marathons), sepsis, trauma and tachydysrhythmias including SVT.
According to the EMS narrative, this patient initially refused hospital transport and advised that he would seek evaluation at a later time with his personal physician. According to the EMS narrative, this patient initially refused hospital transport and advised that he would seek evaluation at a later time with his personal physician.
Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. The TOMAHAWK Investigators.
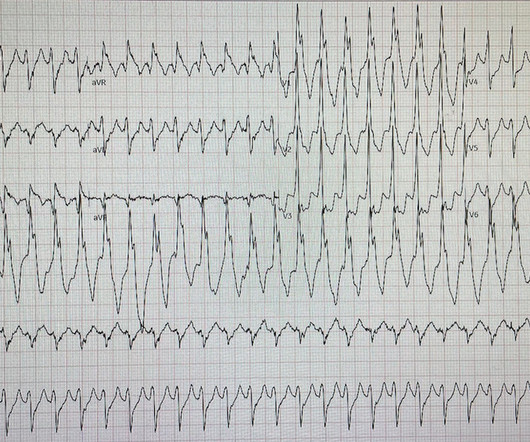
David Didlake EMT-P, RN, ACNP @DidlakeDW An adult male self-presented to the ED with palpitations and the following ECG. I interpreted the ECG as VT with two primary etiological possibilities: 1. Abrupt plaque ulceration of Type 1 ACS leading to VT. The patient was very uncomfortable, dyspneic, and displayed an SpO2 90% on RA.
We’ll keep it short, while you keep that EM brain sharp. The NIHSS cutoff that predicts outcomes is 4 points higher in AC compared with PC infarctions. Median time from ED arrival to diagnosis was 8 hours 24 min in one study, with only 19% being diagnosed within the 4.5-hour Post TW, ed. hour IV thrombolytic window.
However, many institutions’ surgical teams still require or request a formal study over a bedside exam, likely due to a lack of confidence in the accuracy of POCUS, resulting in longer ED stays. ACS surgeons appeared to select surgery as their initial choice substantially more frequently than other subspecialties.
EMS arrived and found him in Ventricular Fibrillation (VF). The patient was brought to the ED and had this ECG recorded: What do you think? Then assume there is ACS. They started CPR. He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. After 1 mg of epinephrine they achieved ROSC.
But this time the Queen gets it wrong (thinks it is not OMI): There were runs of VT: Tha patient arrived in profound shock and had an ED ECG: Now there is some evolution to include the ST elevation (rather than ST depression) in V4-V6. RBBB + LAFB in the setting of ACS is very bad. Posterior and high lateral OMI. Learning Points: 1.
However, RSI has never been shown to reduce the risk of aspiration in the ED (13) or during emergent OR cases (14). While RSI should remain the gold standard in the vast majority of patients in the ED, FI presents an additional technique to mitigate anatomic or physiologic risk. To date, ketamine has been the agent of choice (12).
He presented to EMS with extreme pallor, Levine sign, diaphoresis, bilateral arm pain, and an apprehensive sense of doom. It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). In the case of ACS, the ECG can rapidly change from this. ECG's are difficult.
His parent noticed a dental problem and immediately brought the patient to the ED. Rezaie, MD (Twitter: @srrezaie ) The post Rosh Review EM Scholar Monthly Question appeared first on REBEL EM - Emergency Medicine Blog. The patient was walking his dog when it ran after a squirrel. The physical exam is shown below.
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS. looked at consecutive patients with PE, ACS, or neither.
Written by Pendell Meyers A man in his 40s called EMS for acute chest pain that awoke him from sleep, along with nausea and shortness of breath. Because the most severe LAD OMIs can cause ischemic failure of the RBB and LAF, any patient with ACS symptoms and new RBBB and LAFB with any concordant STE has LAD OMI until proven otherwise.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
AEM May 2022 Guest Skeptic: Dr. Justin Morgenstern is an emergency physician and the creator of the #FOAMed project called First10EM.com Case: A 33-year-old male presents to the emergency department (ED) complaining of abdominal pain. He doesn’t have any specific symptoms today, including no fever, vomiting, diarrhea, or urinary symptoms.
He reported to EMS a medical history of GERD only. 1] Here is the admitting ED ECG after cancellation of Code STEMI. V2 – in the final EMS ECG the ST segment was baseline. V3 – in the final EMS ECG the ST segment was still slightly depressed. The patient continued to verbalize cessation of symptoms while in the ED.
The patient is an adult male with a gunshot wound to the chest, and they’re combative with emergency medical services (EMS). According to a recent study in the Journal of Surgical Research [3] , 44% of all penetrating thoracic trauma patients presented to a non-trauma center (not a level 1 or level 2 ACS defined trauma center).
David Didlake, FF/EMT-P, AG-ACNP @DidlakeDW An elder female presented to the ED with worsening shortness of breath. This should prompt immediate investigation into supply-demand mismatching, or ACS. She was known to have a history of poorly controlled COPD, AFib, and multivessel coronary disease.
Notoriously elusive, with a high misdiagnosis rate, thoracic aortic dissection (AD) can mimic many conditions, including acute coronary syndrome (ACS, the most common), gastroesophageal reflux disease (GERD), stroke, and spinal-cord compression. The patient is admitted for ACS to a cardiologist who says he will see the patient in the morning.
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (ret) @DidlakeDW Expert commentary and peer review by Dr. Steve Smith [link] @smithECGBlog A 57 y/o Female with PMHx HTN, HLD, DM, and current use of tobacco products, presented to the ED with chest discomfort. A 12 Lead ECG was captured on her arrival.
He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines. Here is the initial ED ECG. Patient received 11 shocks by ICD and was in V-fib when EMS arrived.
The machine indicated STEMI (but it barely meets STEMI criteria, if at all) and the patient was brought to the ED: On arrival 20 minutes later the pain had reduced to 1/10 after aspirin, and the patient had repeat ECG at triage: Now the ST segments and T waves have normalized, and the only abnormality is sinus bradycardia and loss of R waves.
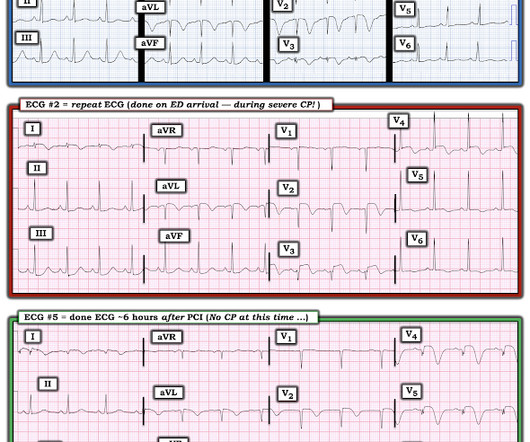
This is acute ACS, but it almost always seen in a pain free state. An ED ECG, if recorded with pain, should show LAD OMI. That said — severe chest pain was present at the time the patient arrived in the ED ( corresponding to the time ECG #2 was recorded ).
PARAMEDIC 3 randomized 6,000 (but they were supposed to get to 15,000) patients with out of hospital arrest from multiple EMS agencies in the UK to either an IO or IV to start. PMID: 39480221 We have 2 studies looking at the same question published in the same edition of the NEJM, so I will tackle them together. ( of the IO group and 5.1%
EMS finds him supine, alert and oriented, and without any gross distress. He advises, however, recurrent syncopal episodes for the past six months, some of which have resulted in ED admission, yet no identifying mechanism could be determined. Chou’s Electrocardiography in Clinical Practice (6th ed). References [1] Surawicz, B.
Here is the first ED ECG recorded, now pain free after sublingual Nitro: There is what appears to be a reperfusion T-wave in I and aVL. EMS arrived — and recorded 2 ECGs. The 3rd tracing in Figure-1 was the initial ED ECG — obtained at a time when the patient's CP had resolved. 14 minutes later — ECG #2 was recorded by EMS.
EMS obtained the following vital signs: pulse 50, respiratory rate 16, blood pressure 96/49. It appears EMS obtained two EKGs, but unfortunately these were not saved in the medical record. The EMS crew was only BLS certified, so EKG interpretation is not within their scope of practice. After all, there is no S wave in lead V3.
Welcome back to the “52 in 52” series. This collection of posts features recently published must-know articles. Today we look at the CENSER trial. vs 48.4% (OR 3.4, 5.53) Takeaways: Positive trial => there was a statistically significant rate of shock control attained with the treatment arm. vs 48.4% (OR 3.4,
The ECG’s were sent to the PCI center, and the providers in the respective ED identified the T wave characteristics mentioned above. Such aggressive investigation was particularly warranted in this case because of symptoms compatible with ACS, as well as an equally frightening revelation of family history. 5] Surawicz, B.
With EMS, patient had a GCS of 3 and was saturating 60% on room air. He improved to 100% with the addition of non-rebreather, however remained altered and was intubated by EMS with ketamine and succinylcholine. EKG on arrival to the ED is shown below: What do you think? or basilar ischemia. Version 2 = 0.0272.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. In our opinion it should not be given in ACS unless you are committed to the cath lab. He was diagnosed as NSTEMI.
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chest pain. Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS.
A 44 year-old male with unknown past medical history came by emergency medical services (EMS) to the emergency department (ED) for an electrical injury and fall from a high voltage electrical pole. Per EMS, the patient was found at the bottom of a high voltage line with diffuse burns and amputation of his left forearm.
Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion. Chou’s Electrocardiography in Clinical Practice, 6th ed. Goldberger’s Clinical Electrocardiography: A Simplified Approach, 9th ed. Annals of Noninvasive Electrocardiology, 18 (1), 21-28.
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. CPR was initiated immediately. It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation.
Submitted by Benjamin Garbus, MD with edits by Bracey, Meyers, and Smith A man in his early 30s presented to the ED with chest pain described as an “explosion" of left chest pressure. Today’s pain lasted around 20 mins, but was severe enough that the patient called EMS. There is no age cut-off for ACS. 1] Wereski, R.,
All you know, back in ED, is that the ETA is 10 minutes, and there is a single stab wound to the chest. The ODP is caught up leaving theatres and has not yet made it down to ED. Back in ED with Ranulf, and pack two has gone through. The trauma call goes out. Would you like a pigtail catheter or a surgical chest tube?
Background Information: Atrial fibrillation with rapid ventricular rate (RVR) is one of the many tachydysrhythmias we encounter in the Emergency Department (ED). The average time to control HR in the IV amiodarone was 1.7h, which is usually the average time for disposition from the ED. Paper: Mason JM, et al.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content