This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
At the time of ED arrival he was alert, oriented, and verbalizing only a headache with a normalized BP. He denied any specific prodrome of gross palpitations, however did endorse feeling quite dizzy just before the event. The ED activated trauma services, and a 12 Lead ECG was captured. The fall was not a mechanical etiology.
That discussion can be deferred until the patient is stable, the risk of such an event is mitigated, and other medications can be given for their withdrawal symptoms and pain. Our experience: Traditionally, ED physicians do not like ordering urine drug screens (UDS). Some patients require re-dosing in the ED. Xylazine toxicity.
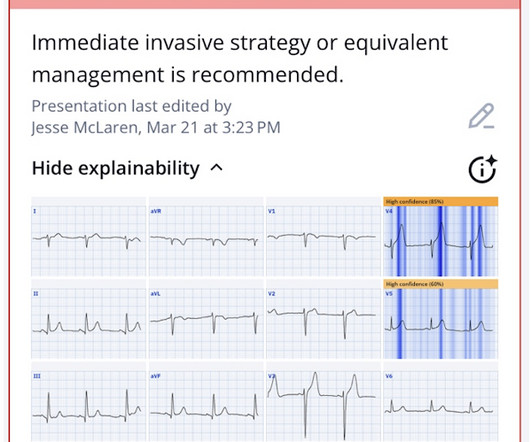
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. There are other reasons aside from ACO for troponin elevations: Type 1: MI due to a spontaneous coronary atherosclerotic event. Send the troponin just to make sure.
Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Case: You are working a shift in your local community emergency department (ED) when a 47-year-old male presents with chest pain.
The trade off to using FI for these challenging airways is the consideration of an aspiration event, the initial indication for RSI. However, RSI has never been shown to reduce the risk of aspiration in the ED (13) or during emergent OR cases (14). To date, ketamine has been the agent of choice (12).
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? The ST depressions in I and aVL have resolved.
[link] Case continued She arrived in the ED and here is the first ED ECG. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. I don't know if her pain was getting better or not.
Because the most severe LAD OMIs can cause ischemic failure of the RBB and LAF, any patient with ACS symptoms and new RBBB and LAFB with any concordant STE has LAD OMI until proven otherwise. Even before looking at the initial ECG — this patient is in a high prevalence group for having an acute event. So the cath lab was activated.
Here is the first ED ECG recorded, now pain free after sublingual Nitro: There is what appears to be a reperfusion T-wave in I and aVL. link] = My Comment by K EN G RAUER, MD ( 11/14 /2023 ): = One of the most helpful clinical clues in support that an acute cardiac event is ongoing — is the finding of " dynamic " ECG changes.
He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines. Here is the initial ED ECG. What do you think? Rhythm : Residents asked me why it is not VT. The QRS is extremely wide.
The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. Smith : As Willy states, ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). She contacted her neighbor, a nurse, for help.
There were zero patients in this study with a "normal" ECG who had any kind of ACS! Figure-1: I've labeled the initial ECG in the ED. KEY Point: All patients who present to the ED for new CP should promptly have a triage ECG recorded, that is then immediately interpreted by the ED physician.
ECG 1 at time zero EARLY REPOLARIZATION ABNORMAL ECG ED final official overread: "early repol vs hyperacute T, minimal changes from previous (previous shown below)" What do YOU think? No wall motion abnormality This shows that significant ACS can have ZERO WMA!! A 70-something y.o. male presents to triage with shortness of breath.
Prior episodes had simply resolved after brief symptoms, but the current episode had lasted for 2 hours without improvement, so she presented to the ED. At triage she stated her pain is still persistent, but it is mildly improved compared to when she decided to come to the ED. No diaphoresis or vomiting.
Because there was proven thrombus (ACS) but the troponin never went above the 99% reference range (and therefore cannot be called MI -- definition of MI requires rise and/or fall of troponin with at least one value above the 99% reference range), this is UNSTABLE ANGINA with ST Elevation. This is not the case.
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Link to abstract Link to full text 2) Use of Morphine in Non-STE-ACS is independently associated with mortality, at odds ratio of 1.4
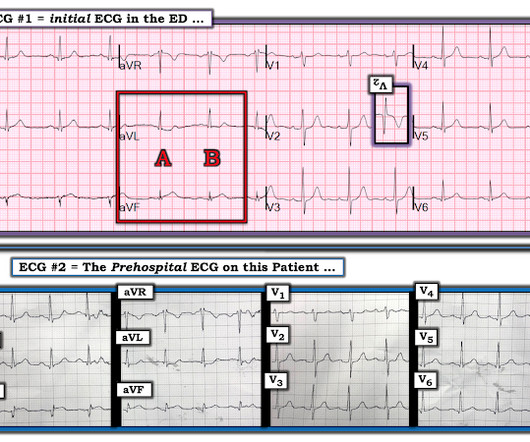
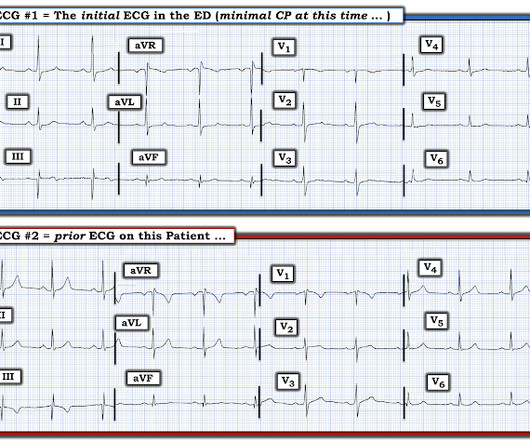
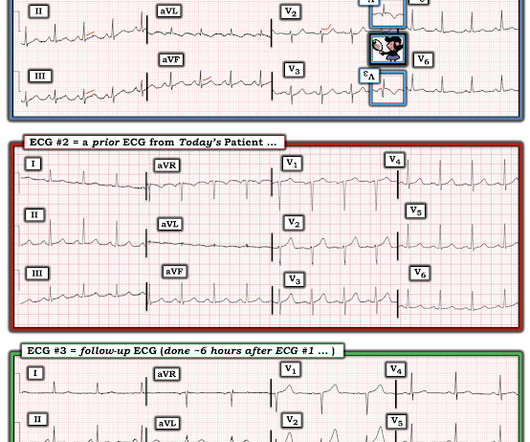
Jerry Jones commented: "Any ST depression on the ECG of a patient with chest pain credible for ACS represents a reciprocal change until proved otherwise." For clarity — I show in Figure-1 the i nitial E CG obtained in the ED ( = E CG # 1 ) — together with the p rehospital E CG that I have pieced together ( = E CG # 2 ).
This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. I was shown today’s initial ECG ( that I’ve reproduced in Figure-1 ) — knowing only that this tracing was from a patient in the ED ( therefore — a patient presumably with some kind of chest discomfort, albeit of unstated duration and severity ).
Written by Jesse McLaren A 75 year-old patient with diabetes and end stage renal disease was sent to the ED after dialysis for three days of nausea, vomiting, loose stool, lightheadedness and fatigue. But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. Below is the 15 lead ECG.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. In our opinion it should not be given in ACS unless you are committed to the cath lab. Unfortunately — 1.5
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Around 19 hours later, he experienced the same pain, which prompted his presentation to the ED.
link] A 30 year-old woman was brought to the ED with chest pain. SCAD isn’t rare, especially in women Historically SCAD had been identified in 22% of ACS cases in women. Pregnancy is not a common cause of SCAD When ACS occurs in the peripartum period, SCAD is responsible in 43% of cases. This is written by Brooks Walsh.
Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion. Whether this represents a potential acute cardiac event would depend on the history, comparison with prior tracings and serial tracings. Chou’s Electrocardiography in Clinical Practice, 6th ed.
Submitted by Dr. George Mastoras (Twitter @georgemastoras), written by Jesse McLaren It’s a busy day in the ED when you’re sent another ECG to sign off from a patient at triage. McLaren — the above demographic for today's patient is typical for a much higher-prevalence group for having SCAD as the cause of their acute event.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin.
ED treatment should focus on airway, breathing, and circulation with consideration for cervical spine protection depending on the circumstances surrounding the event. References Webb AC, Wheeler A, Ricci A, et al. Pediatric near-drowning events: do they warrant trauma team activation? 4 Another study cited only 2.3
A 90 yo with a history of orthostatic hypotension had a near syncopal event followed by chest pain. Chest pain was resolved upon arrival in the ED. Chest pain and possible ischemia were attributed not to ACS, but to transient hypoperfusion from orthostatic hypotension. His previous ECG was normal. What is it? Answer below.
An ECG was recorded quickly on return to the ED: (sorry for poor quality, cannot get originals) What do you think? No obvious adverse events were attributed to the thrombolytics. After a negative noncontrast head CT the next step is looking for a hyperdense basilar artery sign AND to perform a CT cerebral angiogram).
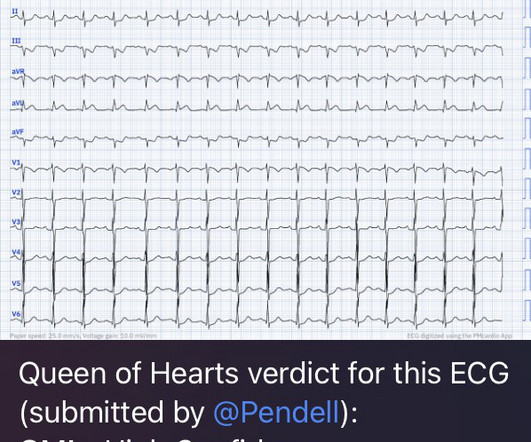
Moreover, the Queen is only supposed to be used with a high pretest probability of ACS/OMI. The patient is a man in his 60s with established severe alcohol use disorder — and epidural abscess being treated with longterm Ciprofloxacin — who presented to the ED following a syncopal episode. Magnesium later resulted at 0.8 As per Drs.
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chest pain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
About an hour later, he was then found on the floor in cardiac arrest in the ED. ST depression maximal in V1-V4, in the context of ACS symptoms and unexplained by QRS abnormality or tachydysrhythmia, should be considered posterior OMI until proven otherwise. His initial troponin T was 15 ng/L (only two hours since pain onset).
FIGURE 1: First ED EKG. FIGURE 2: Baseline ED from 2 months prior. FIGURE 3: Second ED EKG. Considering hyperacute T-waves have been accepted as STEMI equivalents, it is possible that pseudonormalization could gain more recognition as an indicator of ACS. Click to enlarge.) Click to enlarge.) Click to enlarge.)
But there are also hyperacute T waves (HATW) in V4-5, which exclude early repolarization and pericarditis, leaving only LAD occlusion for this patient presenting with classic symptoms of ACS. Chest pain still persists. Cardiology aware. Repeat troponin ordered 0630: lab called for high troponin 3900.
Recall that, in the setting of ACS symptoms, ST depression that are maximal in leads V1-V4 (as opposed to V5 and V6) not attributable to an abnormal QRS complex is specific for OMI. The most recent event had occurred just before being triaged. This pattern is recognizable by the ST depressions maximal in lead V4.
On arrival to the ED, the patient was diaphoretic, tachycardic. I did not think it was due to ACS, but we ordered an ED ECG immediately: What do you think? Under most circumstances — this combination of ECG findings would point to an acute event. and had dilated pupils. He was alert and oriented. both here and here ).
Corroborating this is the subtle ST depression in V2-V3 which is inappropriate for the normal QRS complex, and in the context of ACS, we have shown this is quite specific for posterior OMI. In the context of ACS, ST depression maximal in V1-V4 (rather than V5-V6) not due to a QRS abnormality is specific for posterior OMI.
Case "Male, 43yo, come to ED with Epigastric Pain started 3 hours ago. Remember: these findings above are included as STEMI equivalent findings in the 2022 ACC Expert Consensus Decision Pathway on ACS Patients in the ED. Since then, I started looking for OMI EKG findings and not just STEMI. Risk Factors: High Cholesterol.
The patient has heart failure as a result of this event. They gave him 2 nitroglycerine and transported to the ED. In the ED, the patient was "moaning, writhing in bed, and clutching his chest." A 2nd ED ECG was done at 3 hours after chest pain onset: ST depression maximal in V2-V4 persists, and is actually a bit more profound.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. Takotsubo is a sudden event, not one with crescendo angina. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chest pain.
He still had active pain on arrival to the ED. This is the most important exception to the classic teaching of "diffuse STE without reciprocal depression is less likely ACS, more likely pericarditis". His initial ECG in the ED ( = E CG # 1 ) is shown in Figure-1. Here is his triage ECG: What do you think?
1 The American College of Surgeons’ (ACS) Trauma Quality Improvement Program (TQIP) Massive Transfusion in Trauma Guidelines leave a good amount of flexibility for hospitals regarding transfusion protocols, focusing more on systems-level aspects of designing and implementing MTPs.2,3 ACS TQIP Best Practice Guidelines. 248(3):447-58.
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion).
Results of this study showed that the use of low-dose insulin infusion led to similar clinical outcomes and fewer adverse events compared to the standard-dose insulin infusion. units/kg/hr ) is as efficacious as standard-dose, with fewer adverse events. Garabon JJW, Gunz AC, Ali A, Lim R. years in the non-bougie group.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content