This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Clinical impact: Rather than arguing with the patient about the likelihood of this phenomenon occurring and whether this is a true allergy, the patient is informed that they do not need to immediately start treatment to receive care in the hospital. Our experience: Traditionally, ED physicians do not like ordering urine drug screens (UDS).
A 5-year-old female presented to the emergency department (ED) with a one-year history of gradually increasing anterior neck swelling. She was discharged from the ED on levothyroxine 25 mcg daily with endocrinology outpatient follow-up. The patient had no significant past medical history. Pediatric neck masses. Pediatr Rev.
However, many institutions’ surgical teams still require or request a formal study over a bedside exam, likely due to a lack of confidence in the accuracy of POCUS, resulting in longer ED stays. ACS surgeons appeared to select surgery as their initial choice substantially more frequently than other subspecialties.
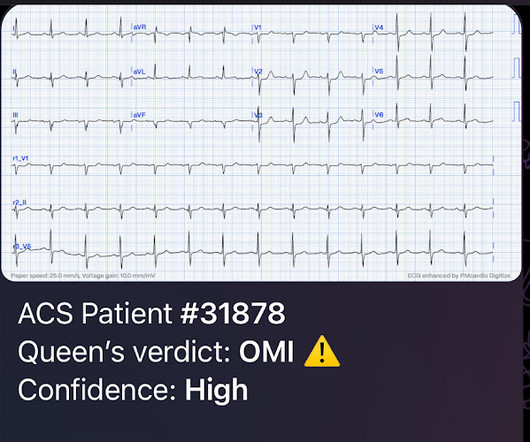
Sent by anonymous, written by Pendell Meyers I received a text with this image and no other information: What do you think? The person I was texting knows implicitly based on our experience together that I mean "Definite posterior OMI, assuming the patient's clinical presentation is consistent with ACS." mm STE in the posterior leads.
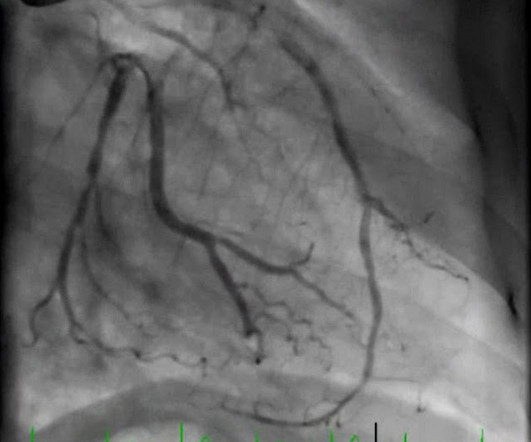
[link] Case continued She arrived in the ED and here is the first ED ECG. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. I don't know if her pain was getting better or not.
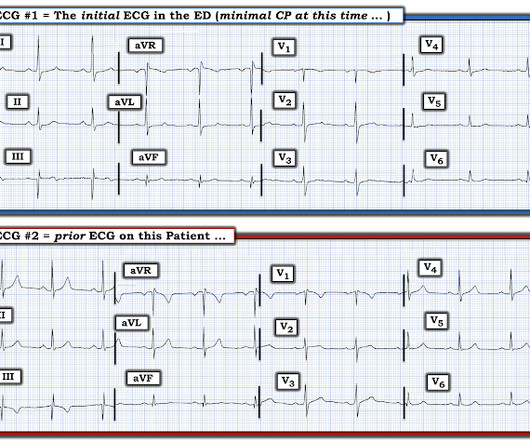
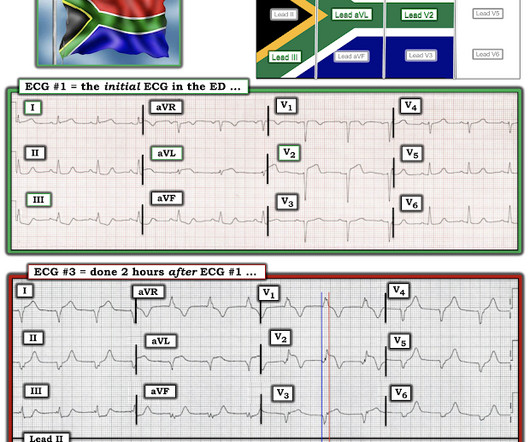
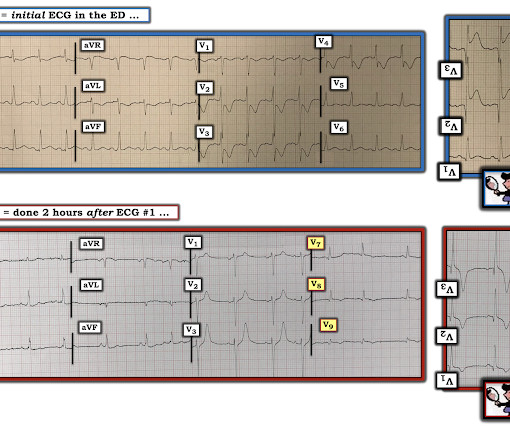
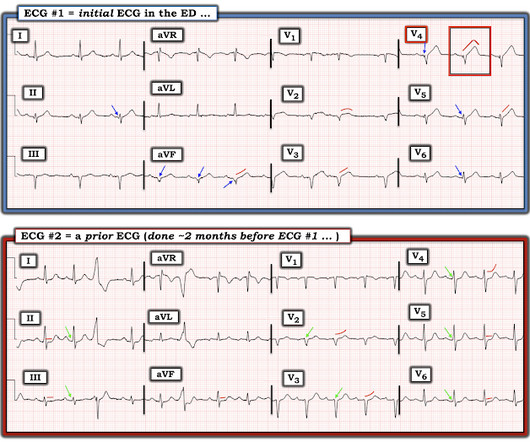
There were zero patients in this study with a "normal" ECG who had any kind of ACS! Figure-1: I've labeled the initial ECG in the ED. KEY Point: All patients who present to the ED for new CP should promptly have a triage ECG recorded, that is then immediately interpreted by the ED physician.
He sent it to me with no other information and I wrote back "100% diagnostic of LBBB with inferior-posterior-lateral OMI" There is atrial paced rhythm with Left Bundle Branch Block (LBBB). The cath report showed: Significant stenosis with subtotal occlusion (99%) in the prox to mid Lcx, culprit of ACS, TIMI flow 1.
I texted this ECG with no information to Dr. Smith, who immediately said: "If CP, then anterior OMI until proven otherwise." References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Am Heart J.
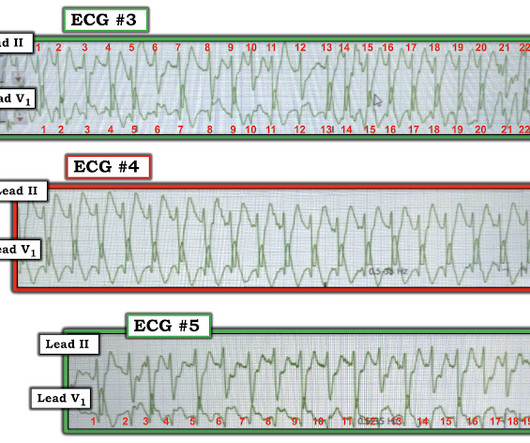
Here is the first ED ECG recorded, now pain free after sublingual Nitro: There is what appears to be a reperfusion T-wave in I and aVL. The 3rd tracing in Figure-1 was the initial ED ECG — obtained at a time when the patient's CP had resolved. Shortly thereafter, on arrival in the ED — ECG #3 was recorded.
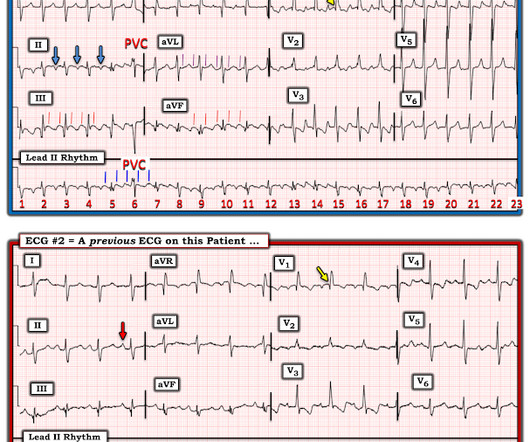
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Around 19 hours later, he experienced the same pain, which prompted his presentation to the ED.
Arch Dis Child Fetal Neonatal Ed. Patterns of parental online health information-seeking behaviour. Arch Dis Child Fetal Neonatal Ed. De Alwis AC, et al. Eur J Pediatr. 2023 Apr 21. Effect of initial and subsequent mask applications on breathing and heart rate in preterm infants at birth. Kuypers KLAM, et al. 2023 Apr 18.
Smith: If this is ACS (a big if), t his is just the time when one should NOT use "upstream" dual anti-platelet therapy ("upstream" means in the ED before angiography). History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Anything more on history?
I did not have more information at the time. To the ED providers, the patient denied CP, SOB, or drug use. This is the ED bedside echo, recorded during ST elevation: Parasternal short axis shows huge concentric LVH. I remained unconvinced that this was due to ACS. Is there a formula to help with this?
Here is his triage ECG: PM Cardio version: With no other information at all, I sent this ECG to Dr. Smith, who replied: "I think it is real. About an hour later, he was then found on the floor in cardiac arrest in the ED. QUESTIONS: About 1 hour after ECG #1 was done — the patient was found on the floor in the ED in cardiac arrest.
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chest pain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
The NIHSS cutoff that predicts outcomes is 4 points higher in AC compared with PC infarctions. While MRI is more resource and time intensive, studies have shown that a 6-minute protocol can give sufficient information to dictate treatment in the right setting. Post TW, ed. hour IV thrombolytic window. Neurohospitalist.
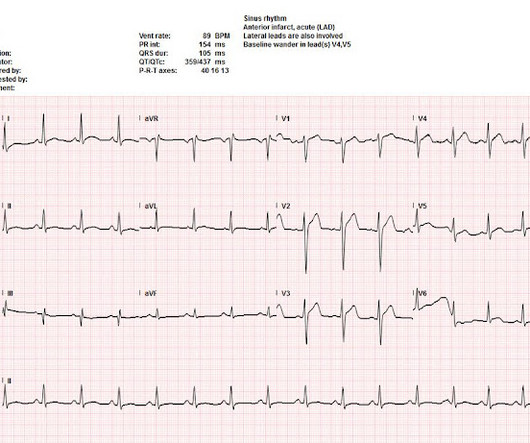
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion).
Background Information: Atrial fibrillation with rapid ventricular rate (RVR) is one of the many tachydysrhythmias we encounter in the Emergency Department (ED). The average time to control HR in the IV amiodarone was 1.7h, which is usually the average time for disposition from the ED. Paper: Mason JM, et al.
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chest pain. I texted this to Dr. Smith without any information, and this was his reply: "This could be pericarditis but probably is normal variant." I do not believe there is any finding here suggestive of OMI.
Corroborating this is the subtle ST depression in V2-V3 which is inappropriate for the normal QRS complex, and in the context of ACS, we have shown this is quite specific for posterior OMI. I sent the ECG with no information to Dr. McLaren, who instantly replied: "RCA?" (he he means, "inferoposterior OMI, so probably RCA occlusion?").
At this point, with the information above, the patient's overall clinical picture could be consistent with either reperfused OMI, or Non-OMI, since both may have absent pain and inverted T waves. CT Coronary angiogram is usually used to make ACS much less likely in the context of a patient who is ruled out for acute MI by troponins.
Meyers : This ECG was texted to me with no clinical information, and my response was: "That looks like a very subtle LAD OMI. Cardiology was called and the patient was taken for urgent catheterization with the time from ED arrival to cath about 1 hour and 45 minutes. Very very subtle one. What happened?"
I saw this before any other information and knew immediately that it represented an LAD occlusion. Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. The 1st “lesson” is, “All bets are off” — when an adult of any age presents to the ED with new-onset chest discomfort.
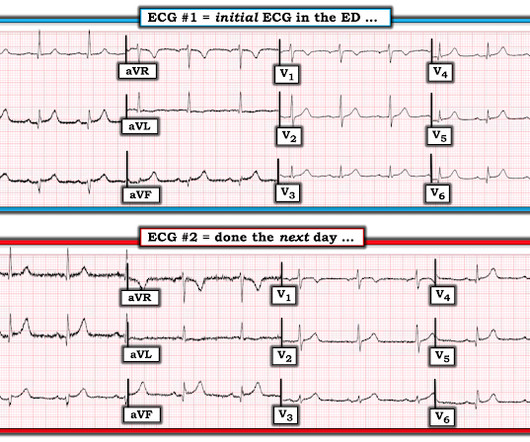
He still had active pain on arrival to the ED. This is the most important exception to the classic teaching of "diffuse STE without reciprocal depression is less likely ACS, more likely pericarditis". His initial ECG in the ED ( = E CG # 1 ) is shown in Figure-1. Here is his triage ECG: What do you think?
I was texted these ECGs by a recent residency graduate after they had all been recorded, along with the following clinical information: A 50-something with no cardiac history, but with h/o Diabetes, was doing physical work when he collapsed. Here is the initial ED ECG: This is pretty obviously and inferior posterior OMI, right?
Recall that, in the setting of ACS symptoms, ST depression that are maximal in leads V1-V4 (as opposed to V5 and V6) not attributable to an abnormal QRS complex is specific for OMI. That this might happen should not be surprising — since the patient's chest pain was already ongoing for 3 hours prior to arrival in the ED.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. Optical coherence tomography, due to its high resolution, may provide additional information [ 10,13 ]. References: 1. Lindahl B, Baron T, Erlinge D, et al.
One case sent by Dr. Sean Rees MD, written by Pendell Meyers, other case by Sam Ghali and Steve Smith Take a look at these two ECGs below from two patients in the ED, first without any clinical context. He had no symptoms of ACS. Full case details and outcomes are below. Case 1: Case 2: Case 1: What do you think? Physician: "No STEMI."
Although not always available a prior ECG is probably the most helpful piece of information in these cases. Most, but not all, ECG “aneurysm morphology” is associated with an actual aneurysm on Echo ( see this case with ED bedside echo ). Beware of ACS presenting with atypical symptoms, including absence of chest pain.
When there is tachycardia, you should doubt the diagnosis of ACS unless it is: a) massive MI with cardiogenic shock and thus poor LV function and poor stroke volume, b) in a patient with previous poor LV function c) combined with other acute pathology causing tachycardia 3. Learning Points: 1.
This ECG was texted to me with no clinical information, with the sender being concerned for possible hyperacute T-waves and STE in the inferior leads. I wouldn't activate the lab for this EKG alone, but if the patient is clinically compatible with ACS you could call a heart alert. Let me know what happens."
Encourage your ED to set up an algorithm that you can follow based on your laboratory’s assay. Low-risk patients do not routinely require stress testing in the ED. You (or someone in your department) needs to know which assay your ED has, and use the appropriate values for that assay. Otherwise, apply a simplified approach.
This ECG is pathognomonic, regardless of any information, prior ECG, etc available: it means the LAD territory is undergoing immediate and hyperacute full thickness infarction, with the most likely etiology being type 1 ACS. Ignoring this truism was the 1st oversight in today's case.
This is her pre-hospital ECG: This is her first ECG in the ED: What do you think? She also received an additional nitro in the ED after receiving aspirin and nitro via EMS. However, this additional information was supportive. Patients like her are the reason we are advocating for a change in the ACS paradigm from STEMI to OMI.
Just so you know this ECG interpretation is not done by the retrospectoscope: I sent it to Dr. Smith without any information, and he immediately responded: "Infero-postero-lateral OMI" The ECG had a computer and final cardiology interpretation of “possible inferior infarct, age undetermined”, because of Q waves.
Written by Pendell Meyers, with some edits by Smith A man in his 40s with many comorbidities presented to the ED with chest pain, hypotension, dyspnea, and hypoxemia. especially given that my first impression was made without the benefit of clinical information. Here is his triage ECG: What do you think? Lots of info here.
This is the initial ED ECG of a 46 year old male with chest pain: The QTc was 420 ST Elevation at 60 ms after the J-point in lead V3 = 2.5 Case 3 I was reading a stack of ECGs yesterday, and saw this one, with no clinical information. Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? QRS V2 = 12.5
The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. What would you do at this time with this information? But pain is an important signal in MI and informs the clinician of the urgency. She contacted her neighbor, a nurse, for help. At midnight.
If this EKG were handed to you to screen from triage without any clinical information, what would you think? showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS. looked at consecutive patients with PE, ACS, or neither.
This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. I sent it to 5 of my OMI friends without any clinical information or outcome and all 5 independently responded with exactly the same diagnosis: "reperfused inferior OMI". There is ischemic ST depression in V4-V6. Figure-1: The initial ECG in today's case.
This is supplied via alternating current (AC), increasing the risk of titanic contraction of skeletal muscle, leading to kids holding on to the electrical power source. AC and DC shocks may result in different injury patterns. In: Walls RM, ed. How does electricity cause harm? Was the voltage high or low (as below)? Culnan, D.M.,
I sent the ECG to Dr. Meyers without any information, and he immediately replied, “inferior OMI.” According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists.
Submitted by Benjamin Garbus, MD with edits by Bracey, Meyers, and Smith A man in his early 30s presented to the ED with chest pain described as an “explosion" of left chest pressure. At the time of arrival to the ED, the patient reported 1/10 chest pain with normal vital signs. There is no age cut-off for ACS. Do NOT use them.
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. CPR was initiated immediately. It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content