This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Our experience: Traditionally, ED physicians do not like ordering urine drug screens (UDS). In our study, we used COWS alone in the ED, which does utilize restlessness, anxiety, and tachycardia as part of the formula, as the sole evaluation tool for tranq dope withdrawal. Some patients require re-dosing in the ED.
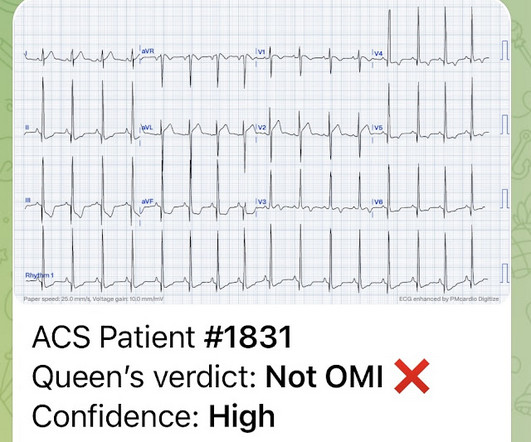
This 29 year old African American patient was found down, unconscious, not breathing and was given 2 mg of intranasal naloxone by a bystander. On arrival to the ED, the patient was diaphoretic, tachycardic. I did not think it was due to ACS, but we ordered an ED ECG immediately: What do you think? and had dilated pupils.
He awoke with naloxone. After discussing all of the above with ED staff, we have made a decision to get stat echocardiogram and assess overall LV function and wall motion abnormalities and defer cath lab activation at the time." The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction.
An 8-year old male with a history of sickle cell anemia presents to the ED for evaluation of fever for 2 days and “feeling like I can’t get a full breath”. 768: Epidemiology of Hospital Based ED Visits due to Sickle Cell Crisis and Acute Chest Syndrome in Kids. Chinawa JM, Ubesie AC, Chukwu BF, Ikefuna AN, Emodi IJ. C or 100.4
Haematology specialist clinics are key to manage the chronic side of the disease, while ED doctors should be able to act rapidly on the common acute emergencies. with thanks A 15-month-old Kenyan boy presents to ED with right hand swelling. A 10-year-old boy with known SCA presents to ED due to severe pain in the legs.
A 33-year-old male with a history of drug use presented to the emergency department (ED) for extreme agitation after receiving two doses of 2 mg naloxone by EMS for respiratory depression. If available, an in-house ED pharmacist is an incredible resource for guidance when there are questions regarding pharmacologic management.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












Let's personalize your content