This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Encourage your ED to set up an algorithm that you can follow based on your laboratory’s assay. Low-risk patients do not routinely require stress testing in the ED. You (or someone in your department) needs to know which assay your ED has, and use the appropriate values for that assay.
At the time of ED arrival he was alert, oriented, and verbalizing only a headache with a normalized BP. The ED activated trauma services, and a 12 Lead ECG was captured. This was deemed “non-specific” by the ED physicians. Thus, the ED admission ECG changes cannot be blamed on LVH. The fall was not a mechanical etiology.
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
Trauma season is at hand and like all other pediatric emergency departments in the country, we find our ED breaking ( pun intended ) at the seams with orthopedic injuries. We see all different flavors of upper extremity injuries. The minority of parents would have wanted clinic follow up (6%) and reimaging (14%).
Case: You are working a busy shift in a rural emergency department (ED) and your excellent Family Medicine trainee presents a case of a 63-year-old woman with chest pain and some intermittent radiation into the inter-scapular region. The patient has no specific risk factors for acute coronary syndrome (ACS) or dissection.
Cardiology consult note written around that time documents that "Pain improved with NTG, morphine in ED but still present." As a result, even before looking at this patient's initial ECG — he falls into a high -prevalence likelihood group for ACS ( for an A cute C oronary S yndrome ). Repeat cTnI drawn at around 8 AM was 3.910 ng/mL.
European Journal of Internal Medicine , [link] You can listen to my 27-minute rant on Youtube here: [link] This multinational trial looked at a three-pronged diagnostic protocol in the ED for adults with suspected acute aortic syndromes. The protocol used the ADD score, a POCUS echo protocol and D-dimer to try and exclude AAS in the ED.
In the age of high sensitivity troponins and the HEART pathway, which patients are safe to discharge home from the ED? What are the most useful historical factors to increase and decrease your pretest probability for ACS? Which cardiac risk factors have predictive value for ACS? Which delta troponin is best - 1hr, 2hr or 3hr?
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. Type 2 MI is common in the ED and can result from vigorous exercise (common in athletes after marathons), sepsis, trauma and tachydysrhythmias including SVT.
You turn to the attending and ask, “do you really think this could be acute coronary syndrome (ACS)?” ACS is usually amongst this differential, as cardiovascular disease is a leading cause of morbidity and mortality in this population. The proportion of patients with ACS at the index visit or within 30 days. *
A 5-year-old female presented to the emergency department (ED) with a one-year history of gradually increasing anterior neck swelling. She was discharged from the ED on levothyroxine 25 mcg daily with endocrinology outpatient follow-up. The patient had no significant past medical history. Abdominal : Soft. No distention or tenderness.
Other causes of sickling: acidosis, dehydration, inflammation, infection, fever, and blood stasis Sickling leads to vascular occlusion, end-organ ischemia, and decreased RBC lifespan, which, in turn, leads to pain crisis, acute anemia, sequestration, infection, and acute chest syndrome (ACS.) Each episode of ACS has a 9% mortality rate.
The patient was brought to the ED and had this ECG recorded: What do you think? Then assume there is ACS. After 1 mg of epinephrine they achieved ROSC. Total prehospital meds were epinephrine 1 mg x 3, amiodarone 300 mg and 100 mL of 8.4% sodium bicarbonate. And what do you want to do? Cardiac arrest #3: ST depression, Is it STEMI?
Although the attending crews did not consider the ECG pathognomonic for occlusive thrombosis, they nonetheless considered the patient high-risk for ACS and implored him to reconsider. Here is the final ECG just prior to ED transfer. Moreover, he had no pertinent medical history to report in terms of CAD, HTN, HLD, or DM, for example.
Sickling leads to vascular occlusion, end-organ ischemia, and decreased RBC lifespan, which, in turn, leads to pain crisis, acute anemia, sequestration, infection, and acute chest syndrome (ACS). ACS is lung injury due to vaso-occlusion in the pulmonary vasculature; many with ACS will have a concomitant vaso-occlusive pain crisis.
Case: A 46-year-old female presents to the emergency department (ED) with sudden onset, severe right flank pain. Delays in providing adequate analgesia leads to poorer patient outcomes, prolonged ED length of stay and reduced patient satisfaction (17, 18). AEM Feb 2021. Reference: Brichko et al.
Case: You are working a shift in your local community emergency department (ED) when a 47-year-old male presents with chest pain. Background: Chest pain is one of the most common presentations to the ED. In prior decades nearly all patients presenting to EDs with chest pain were admitted to hospital. AEM June 2022.
But this time the Queen gets it wrong (thinks it is not OMI): There were runs of VT: Tha patient arrived in profound shock and had an ED ECG: Now there is some evolution to include the ST elevation (rather than ST depression) in V4-V6. RBBB + LAFB in the setting of ACS is very bad. There is STE in aVR. Posterior and high lateral OMI.
However, RSI has never been shown to reduce the risk of aspiration in the ED (13) or during emergent OR cases (14). While RSI should remain the gold standard in the vast majority of patients in the ED, FI presents an additional technique to mitigate anatomic or physiologic risk.
showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS. In this study, (quote) "negative T waves in leads III and V 1 were observed in only 1% of patients with ACS compared with 88% of patients with Acute PE (p less than 0.001).
He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP). She arrives in the emergency department (ED) with decreased level of consciousness and shock.
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (ret) @DidlakeDW Expert commentary and peer review by Dr. Steve Smith [link] @smithECGBlog A 57 y/o Female with PMHx HTN, HLD, DM, and current use of tobacco products, presented to the ED with chest discomfort. A 12 Lead ECG was captured on her arrival.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? The ST depressions in I and aVL have resolved.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). ACE inhibitors, or potassium-sparing diuretics), are particularly susceptible. In the case of ACS, the ECG can rapidly change from this. Chou's Electrocardiography in Clinical Practice, 6th ed.
David Didlake, FF/EMT-P, AG-ACNP @DidlakeDW An elder female presented to the ED with worsening shortness of breath. This should prompt immediate investigation into supply-demand mismatching, or ACS. She was known to have a history of poorly controlled COPD, AFib, and multivessel coronary disease.
George Mastoras (Twitter @georgemastoras), written by Jesse McLaren It’s a busy day in the ED when you’re sent another ECG to sign off from a patient at triage. A healthy 45-year-old female presented with chest pain, with normal vitals. The computer interpretation was “ST elevation, consider early repolarization, pericarditis or injury.”
Notoriously elusive, with a high misdiagnosis rate, thoracic aortic dissection (AD) can mimic many conditions, including acute coronary syndrome (ACS, the most common), gastroesophageal reflux disease (GERD), stroke, and spinal-cord compression. The patient is admitted for ACS to a cardiologist who says he will see the patient in the morning.
The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. Smith : As Willy states, ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). She contacted her neighbor, a nurse, for help. At midnight.
The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). Those who make it to the ED usually have transient occlusions with reperfusion.
Upon arrival in the emergency department (ED), the patient is incoherently speaking, has a pulse of 135 beats per minute, blood pressure of 85/50 mm Hg, and an obvious open wound in their left mid-axillary line at the level of the nipple. Journal of Trauma and Acute Care Surgery. We did the session over zoom as an SGEM Journal Club.
[link] Case continued She arrived in the ED and here is the first ED ECG. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. I don't know if her pain was getting better or not.
He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines. Here is the initial ED ECG. What do you think? Rhythm : Residents asked me why it is not VT. The QRS is extremely wide.
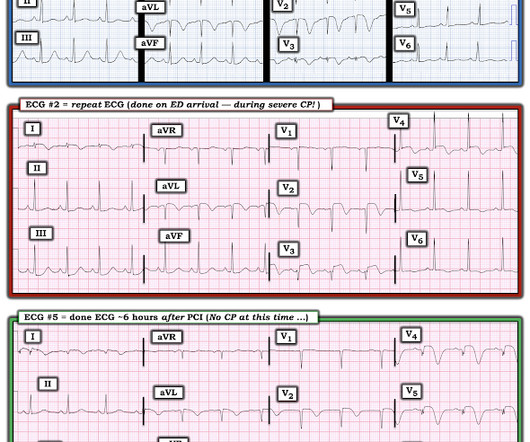
This is acute ACS, but it almost always seen in a pain free state. An ED ECG, if recorded with pain, should show LAD OMI. That said — severe chest pain was present at the time the patient arrived in the ED ( corresponding to the time ECG #2 was recorded ). Low TMP grade correlates very well with resolution of ST Elevation.
Key: Consider eclampsia in any pregnant and postpartum woman presenting to the ED, especially in patients with symptoms such as headache, confusion/altered mental status, vision changes, and hypertension. ED Evaluation: Assessment focuses on looking for complications and mimics. This is not borne out in the literature.
There were zero patients in this study with a "normal" ECG who had any kind of ACS! Figure-1: I've labeled the initial ECG in the ED. KEY Point: All patients who present to the ED for new CP should promptly have a triage ECG recorded, that is then immediately interpreted by the ED physician. Deutch et al.
Episode 108: Unexplained Sinus Tachycardia Mental Model Background: When a patient in the ED has sinus tachycardia our job as emergency physicians is to identify and treat of the underlying pathology. Today on the emDOCs cast Brit Long interviews Zachary Aust on the use of a mental model for patients with unexplained sinus tachycardia.
He advises, however, recurrent syncopal episodes for the past six months, some of which have resulted in ED admission, yet no identifying mechanism could be determined. Steve Smith [link] @SmithECGblog A 72 y/o Male experiences a syncopal episode while seated. It’s reported that he regained consciousness after 30 seconds, approximately.
1] Here is the admitting ED ECG after cancellation of Code STEMI. The patient continued to verbalize cessation of symptoms while in the ED. A 56 y/o Male called 911 from his hotel room in the early morning hours after abruptly awakening from sleep with crushing chest discomfort and difficulty breathing. However, in this context (i.e.
Justin Morgenstern is an emergency physician and the creator of the #FOAMed project called First10EM.com Case: A 33-year-old male presents to the emergency department (ED) complaining of abdominal pain. He states he has had the same pain for more than 10 years, and no one has ever been able to figure out what is going on.
This is supplied via alternating current (AC), increasing the risk of titanic contraction of skeletal muscle, leading to kids holding on to the electrical power source. Up to 5% of burns occur secondary to electrical injuries, and this rises to 27% in developing countries. Was the voltage high or low (as below)? Was there any syncope ?
The ECG’s were sent to the PCI center, and the providers in the respective ED identified the T wave characteristics mentioned above. He reports to staff that for the past two months, approximately, he has experienced intermittent dyspnea on exertion when walking the dog, particularly when scaling an incline. Does the ECG normalize?
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Link to abstract Link to full text 2) Use of Morphine in Non-STE-ACS is independently associated with mortality, at odds ratio of 1.4
This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. I was shown today’s initial ECG ( that I’ve reproduced in Figure-1 ) — knowing only that this tracing was from a patient in the ED ( therefore — a patient presumably with some kind of chest discomfort, albeit of unstated duration and severity ).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















































Let's personalize your content