This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
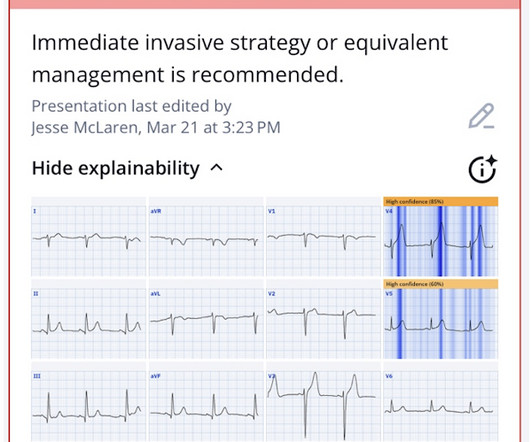
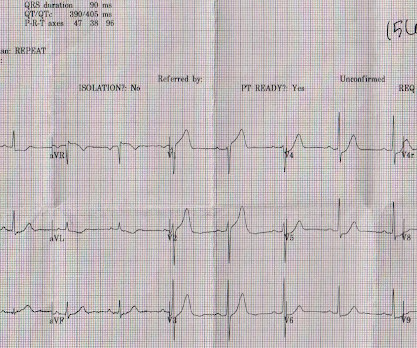
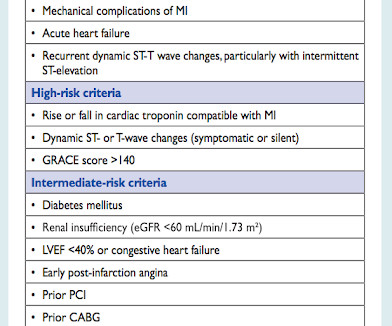
Because the most severe LAD OMIs can cause ischemic failure of the RBB and LAF, any patient with ACS symptoms and new RBBB and LAFB with any concordant STE has LAD OMI until proven otherwise. There is no recognition of STEMI equivalency in this setting in the USA guidelines currently. So the cath lab was activated.
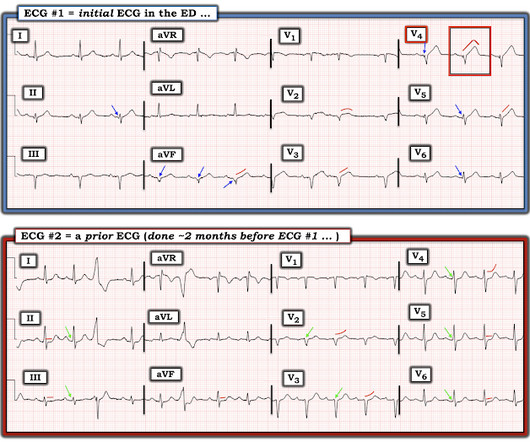
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. But there are also hyperacute T waves (HATW) in V4-5, which exclude early repolarization and pericarditis, leaving only LAD occlusion for this patient presenting with classic symptoms of ACS.
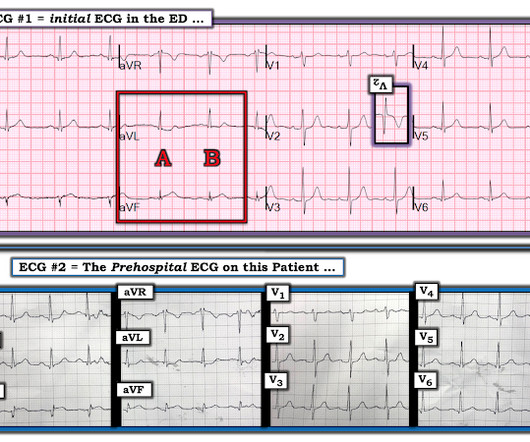
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
The person I was texting knows implicitly based on our experience together that I mean "Definite posterior OMI, assuming the patient's clinical presentation is consistent with ACS." The interventional cardiologist then canceled the activation and returned the patient to the ED without doing an angiogram ("Not a STEMI").
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? The ST depressions in I and aVL have resolved.
Although the attending crews did not consider the ECG pathognomonic for occlusive thrombosis, they nonetheless considered the patient high-risk for ACS and implored him to reconsider. A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. The pathology is now painfully evident.
The patient was brought to the ED and had this ECG recorded: What do you think? Then assume there is ACS. Cardiac arrest #3: ST depression, Is it STEMI? After 1 mg of epinephrine they achieved ROSC. Total prehospital meds were epinephrine 1 mg x 3, amiodarone 300 mg and 100 mL of 8.4% sodium bicarbonate.
There were zero patients in this study with a "normal" ECG who had any kind of ACS! So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. Deutch et al.
He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP). She arrives in the emergency department (ED) with decreased level of consciousness and shock.
[link] Case continued She arrived in the ED and here is the first ED ECG. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. I don't know if her pain was getting better or not.
The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI."
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. It’s unclear if the paramedic ECGs were seen or missed in the ED. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. At this point the emergency physician asked for a stat cardiology consult.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). There is mixed overlap of ST-segment elevation (STE), ST-segment depression (STD), Hyperacute T waves (HATW), and deWinter pattern (which the ACC regards as a STEMI-equivalent but is better suited under the blanket of OMI).
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS. Kosuge et al. Witting et al.
This is a 45 yo male who had an inferior STEMI 6 months prior, was found to have severe LAD and left main disease, and was supposed to be set up for CABG a few weeks later, but did not follow up. But it could be anterior STEMI. 40% of anterior STEMI has upward concavity in all of leads V2-V6. is likely anterior STEMI).
Written by Jesse McLaren A 75 year-old patient with diabetes and end stage renal disease was sent to the ED after dialysis for three days of nausea, vomiting, loose stool, lightheadedness and fatigue. But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. Below is the 15 lead ECG.
Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Day 12 ECG: FINAL DIAGNOSIS: "NSTEMI" Despite the fact that his day 4 ECG easily meets STEMI criteria, the patient is diagnosed as NSTEMI. Setting – large, academic, suburban ED. Am Heart J.
BP 142/100 HR 90 RR 16 (BBS CTA) SpO2 99 (RA) Dstick 110 My colleagues noted the ST-depression in the respective leads, as well, and STEMI activated to the nearest PCI center. 1] Here is the admitting ED ECG after cancellation of Code STEMI. The patient continued to verbalize cessation of symptoms while in the ED.
This is as clear a STEMI as you can get. Now, it is true that shortly after a non-ACS cardiac arrest, there can be transient diffuse ST depression, but not ST elevation in a coronary distribution, and there should not be a wall motion abnormality. So this is classic inferoposterior STEMI on the ECG but is NOT acute coronary syndrome!
He had an immediate ED ECG: There is artifact, but the findings appear to be largely gone now The diagnosis is acute MI, but not STEMI. See this post on the (Five primary patterns of ischemic ST depression, without ST elevation) Because of the dynamic ACS, we activated the cath lab in the middle of the night.
A 36 yo male smoker presented to the ED with chest pain. You can see how V1, V2, aVR, and V4R would have ST elevation in either a right ventricular STEMI or with a septal STEMI, and how lateral leads, and even posterior leads, would have reciprocal ST depression. See more on STE in aVR in anterior STEMI, below.
The Queen of Hearts agrees: Here the Queen explains why: However, it was not interpreted correctly by the providers: ED interpretation of ECG: "paced rhythm, LBBB but no STEMI pattern." Most large STEMI have peak troponin I in the 20.0 There are hyperacute T-waves in V5 and V6. Next trop in AM. Peak trop 257.97 ng/mL - 80.0
Written by Bobby Nicholson What do you think of this “STEMI”? EKG on arrival to the ED is shown below: What do you think? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). or basilar ischemia.
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? He was found in ventricular fibrillation and defibrillated, then brought to a local ED which does not have a cath lab. Here is the initial ED ECG: This is pretty obviously and inferior posterior OMI, right? It is a STEMI equivalent.
Furthermore, the term "STEMI equivalent" has no reliable or definable meaning except between two practitioners who both agree on the list of entities that they believe are STEMI equivalents and can agree on how to identify it. Obvious inferoposterior STEMI. J ACC 61(4):e78-140; page e83.
He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. Sensitivity was 87% for OMI in our validation study (it was 34% for STEMI criteria). So it can miss some OMI.
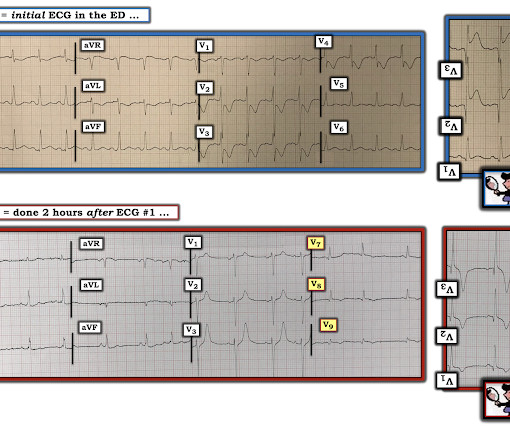
The first (and only) ED ECG is here: QTc 386. Serial ECGs demonstrated dynamic changes diagnostic of ACS (transient STEMI) 4. Finally, Transient STEMI should be taken emergently to the cath lab. Normalization of Diagnostic For STEMI Prehospital ECG with Nitroglycerin Therapy. Most ST elevation is resolved.
Here was his initial ED ECG: There is atrial fibrillation with a rapid ventricular response. Does this patient have ACS? He did not have ACS. We found that 38% of out of hospital ventricular fibrillation was due to STEMI. The remainder were due to other etiologies, (including NonSTEMI ACS). Learning Points: 1.
Jerry Jones commented: "Any ST depression on the ECG of a patient with chest pain credible for ACS represents a reciprocal change until proved otherwise." This algorithm called it a STEMI. Yet it gave a diagnosis of STEMI. This is, in effect, a transient STEMI 2. Learning points 1. They may be helpful.)
ECG 1 at time zero EARLY REPOLARIZATION ABNORMAL ECG ED final official overread: "early repol vs hyperacute T, minimal changes from previous (previous shown below)" What do YOU think? Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Is it normal STE? This is a "Transient OMI".
I delved into his reasons for arriving so late after onset, thinking that perhaps the pain had only recently increased, or that it had been intermittent until now, but he confirmed that it was 14 hours of constant pain and it was his significant other who insisted that he go to the ED. The "criteria" for posterior STEMI are 0.5
Only very slight STE which does not meet STEMI criteria at this time. I am immediately worried that this OMI will not be understood, for many reasons including lack of sufficient STE for STEMI criteria, as well as the common misunderstanding of "no reciprocal findings" which is very common with this particular pattern.
Prior episodes had simply resolved after brief symptoms, but the current episode had lasted for 2 hours without improvement, so she presented to the ED. At triage she stated her pain is still persistent, but it is mildly improved compared to when she decided to come to the ED.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. His response: “subendocardial ischemia. Anything more on history? POCUS will be helpful.”
Submitted by Dr. George Mastoras (Twitter @georgemastoras), written by Jesse McLaren It’s a busy day in the ED when you’re sent another ECG to sign off from a patient at triage. Whereas SCAD is found in ~1-4% of all angiograms performed for ACS — this percentage increases to over 30% in middle-aged women.
The ECG’s were sent to the PCI center, and the providers in the respective ED identified the T wave characteristics mentioned above. STEMI was activated and the patient went to Cath on arrival. Chou’s Electrocardiography in Clinical Practice (6th ed). Conjecture aside, I believe the lesson here, ultimately, is serial ECG’s.
This post will focus on the key parts of the guideline that affect ED evaluation and management. Editorial Comment: ECPR may be considered in patients refractory to standard ACS in the right situation. Editorial Comment : Yes to PCI after arrest with STEMI on ECG. COR 2a, LOE B-R. COR 3, No benefit, LOE B-R.
Figure 1-1 My colleague, a faithful student of ECG interpretation, handed me the tracing and said that it warranted STEMI activation because of apparent terminal QRS distortion (TQRSD) in V2. Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion.
She was hypotensive in the ED and her bedside echo showed a normal RV and LV. Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR. Also note that they allow ST depression c/w posterior MI to be a STEMI equivalent.
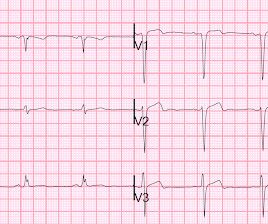
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Around 19 hours later, he experienced the same pain, which prompted his presentation to the ED.
An ECG was recorded quickly on return to the ED: (sorry for poor quality, cannot get originals) What do you think? Is this inferor STEMI? Atrial Flutter with Inferior STEMI? The EM provider asked if the cardiologist thought it was a "STEMI." There is a narrow complex regular rhythm at a rate of approximately 120 bpm.
Smith and Meyers answer: First , LM occlusion is uncommon in the ED because most of these die before they can get a 12-lead recorded. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery? The pattern seen may, or may not, be unique to left main occlusion. TIMI 0/1 flow).(61,62)
This meets "STEMI criteria" However, there is very high voltage, with a very deep S-wave in V2 and tall R-wave in V4. The morphology is not right for STEMI. My interpretation: LVH with secondary ST-T abnormalities, exaggerated by stress, not a STEMI. To the ED providers, the patient denied CP, SOB, or drug use.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content