This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Bupe Allergy Buprenorphine induction has been the mainstay of emergencydepartment treatment of opioid use disorder for more than a decade [11, 12]. That discussion can be deferred until the patient is stable, the risk of such an event is mitigated, and other medications can be given for their withdrawal symptoms and pain.
Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Guest Skeptic: Dr. Corey Heitz is an emergency physician in Roanoke, Virginia. He is also the CME editor for Academic Emergency Medicine. Guest Skeptic: Dr. Corey Heitz is an emergency physician in Roanoke, Virginia.
Myth 1 Absence of Classic Chest Pain obviates the need for ACS work up The absence of chest pain in no way excludes the diagnosis of ACS. Around 33-50% of the patients with ACS present to the hospital without chest pain. Ann Emerg Med 2002; 40:180–6. Heart 2001; 86:494–8. Gupta M, Tabas JA, Kohn MA.
A 41-year-old male who presents to the emergencydepartment with chest pain. The faculty physician thought this is highly likely to be ACS. I do not think it is possible for a 2nd trop to remain undetectable in a patient then goes on to rule in for acute MI, unless there is a 2nd event. No shortness of breath.
Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? Diagnosis of Type I vs. Type II Myocardial Infarction in EmergencyDepartment patients with Ischemic Symptoms (abstract 102). Annals of Emergency Medicine 2011; Suppl 58(4): S211. Assuming that was indeed a culprit, then this was ACS.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. Upon arrival to the emergencydepartment, a senior emergency physician looked at the ECG and said "Nothing too exciting."
The trade off to using FI for these challenging airways is the consideration of an aspiration event, the initial indication for RSI. However, RSI has never been shown to reduce the risk of aspiration in the ED (13) or during emergent OR cases (14). Desaturation can lead to hypoxia and adverse events. Int J Emerg Med.
This was sent by anonymous The patient is a 55-year-old male who presented to the emergencydepartment after approximately 3 to 4 days of intermittent central boring chest pain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin. It is unknown when this pain recurred and became constant.
, tells us that we physicians do not need to even look at this ECG until the patient is placed in a room because the computer says it is normal: Validity of Computer-interpreted “Normal” and “Otherwise Normal” ECG in EmergencyDepartment Triage Patients I reviewed this article for a different journal and recommended rejection and it was rejected.
Optimally, bystander CPR, including the administration of rescue breaths, should be initiated prior to arrival of emergency medical services. 3 Once the patient arrives in your emergencydepartment, a rapid review of the patient’s status and results of resuscitative efforts should be performed. Pediatr Emerg Med Pract.
A 35-year-old male presented to the emergencydepartment complaining of chest pain that started 1.5 5 Studies looking at this phenomenon in the emergencydepartment setting for patients presenting with chest pain are lacking. Dr. Young is an emergency physician at Saint Francis Hospital and Medical Center, Hartford, Conn.
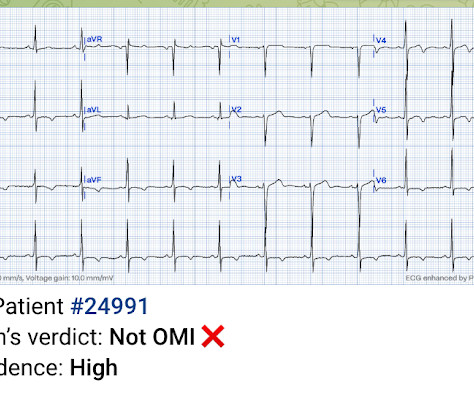
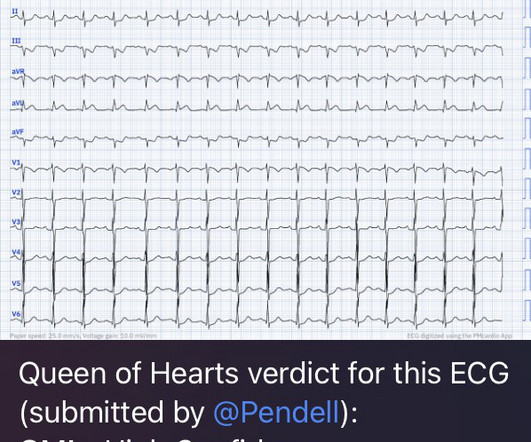
A man in his 60s with a history of severe alcohol use disorder and epidural abscess on long-term ciprofloxacin presented to the emergencydepartment after an episode of syncope while standing in line at a grocery store. Moreover, the Queen is only supposed to be used with a high pretest probability of ACS/OMI.
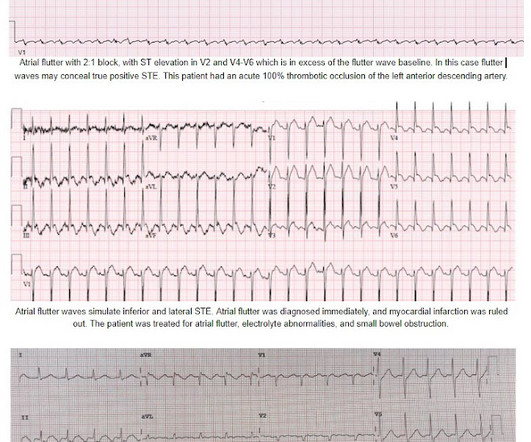
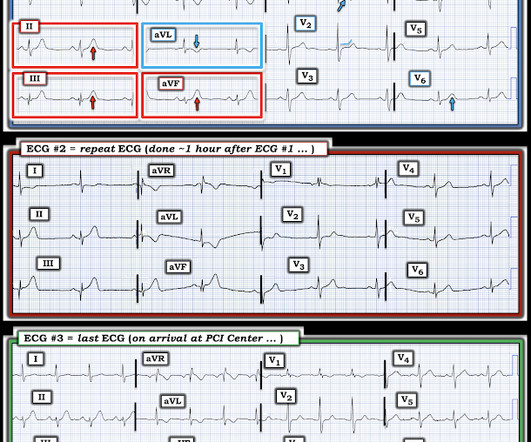
On arrival to the PCI center's EmergencyDepartment, the receiving team recorded an ECG on arrival: Persistent atrial flutter, however this time the QRS occurs on a slightly different portion of the flutter wave. No obvious adverse events were attributed to the thrombolytics. There was again no intracranial hemorrhage.
While in the emergencydepartment, he undergoes an additional ECG: 00:49 - Not much change Second ECG with measurements and calculations Magnified view of second ECGs measurements and calculation It is still "negative" for LAD occlusion (less than 23.4) Use caution when prescribing opioids to patients concerning for ACS.
Results of this study showed that the use of low-dose insulin infusion led to similar clinical outcomes and fewer adverse events compared to the standard-dose insulin infusion. units/kg/hr ) is as efficacious as standard-dose, with fewer adverse events. Garabon JJW, Gunz AC, Ali A, Lim R. Prehosp Emerg Care.
titled “Intubation Practices and Adverse Peri-intubation Events in Critically Ill Patients from 29 Countries,” at least one major critical event occurred after intubation in 45.2% The higher the shock index, the more likely adverse events are to occur; such as hypotension or cardiac arrest. Up to 44% per other sources [12].
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergencydepartment with substernal chest pain for 3 hours prior to arrival. The most recent event had occurred just before being triaged. Triage EKG: What do you think?
I finished my residency of Emergency Medicine and I’m working at a great EmergencyDepartment here in Brazil. Remember: these findings above are included as STEMI equivalent findings in the 2022 ACC Expert Consensus Decision Pathway on ACS Patients in the ED.
He had no symptoms of ACS. The remainder of his EmergencyDepartment stay was uneventful. Here is the clinical informaton on ECG 2: A man in his 50s presented to the EmergencyDepartment with acute chest pain that started within the past few hours. QOH: "OMI High confidence". Physician interpretation: "No STEMI."
She was brought to the EmergencyDepartment and this ECG was recorded while she was still feeling nauseous but denied chest pain, shortness of breath, or other symptoms: What do you think? I wouldn't activate the lab for this EKG alone, but if the patient is clinically compatible with ACS you could call a heart alert.
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in EmergencyDepartment COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. of Cardiology AC, Others. Cardiac Troponin Testing in Patients with COVID-19: A Strategy for Testing and Reporting Results.
IIa C Pre-hospital logistics Management Recommendation Level of evidence The pre-hospital care of STEMI patients should be organized regionally (including all components from the emergency medical dispatch to catheterization laboratory) in order to provide reperfusion therapy as early as possible. mmol/L or <_ 70 mg/dL) should be avoided.
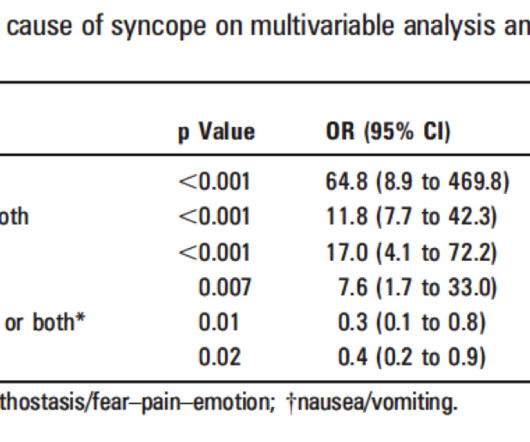
(full text link) Presence of any one of these 8 criteria had 97% sensitivity and specificity of 62% for adverse outcomes: 1) Signs of Acute Coronary Syndrome (ACS), 2) conduction disease, 3) worrisome cardiac history, (eg. The ROSE (Risk Stratification of syncope in the emergencydepartment) Study.
Case submitted and written by Dr. Mazen El-Baba and Dr. Emily Austin, with edits from Jesse McLaren A 50 year-old patient presented to the EmergencyDepartment with sudden onset chest pain that began 14-hours ago. The pain improved (6/10) but is persisting, which prompted him to visit the EmergencyDepartment. Shroff, G.
Whilst the incidence of adverse events was low in this meta-analysis, this reflects adverse event reporting in RCTs rather than reality. A Randomized Trial of Single-Dose Oral Dexamethasone Versus Multidose Prednisolone for Acute Exacerbations of Asthma in Children Who Attend the EmergencyDepartment. Arch Dis Child.
6 Prolonged down time from falls, usually in the elderly Incidence is difficult to ascertain due to broad definition and that events that cause crush injuries are rather rare. J Emerg Med. Goodman AD, Got CJ, Weiss AC. Clinical spectrum of rhabdomyolysis presented to pediatric emergencydepartment. Int J Emerg Med.
There were trends toward larger infarct size with delayed angiography, both by cMR and integral high-sensitivity troponin concentration, as well as toward higher rate of major adverse cardiovascular events (MACE) (8.5 vs. 2.9%; P = 0.28) in the delayed group. paramedic transportation to the ED as “chest pain, STEMI negative” 2. Kontos et al.
Am J Emerg Med. Chinawa JM, Ubesie AC, Chukwu BF, Ikefuna AN, Emodi IJ. Intranasal fentanyl and discharge from the emergencydepartment among children with sickle cell disease and vaso-occlusive pain: A multicenter pediatric emergency medicine perspective. C or 100.4 mg/kg, max 0.4 2022 Aug;58:235244. Am J Hematol.
Opioids do not cause ACS but they can exacerbate hypoxia in patients with ACS. A 6-year-old girl from Saudi Arabia was referred by her General Practitioner to the local emergencydepartment. Mechanical or non-invasive ventilation : children with ACS may require ventilatory support.
Another EKG, shown with a V1 rhythm strip, was recorded in the emergencydepartment: EKG 3, 1930 There appears again to be some reperfusion since the last EKG, as the T waves in inferior leads have deflated slightly. When the patient finally arrived to the PCI-capable hospital, his pain had reportedly improved, but not resolved.
The ECG was transmitted to the Emergency Medicine physician who recognized inferior and posterior OMI findings, and confirmed that the patient has potential ACS symptoms. EMS gave aspirin and nitroglycerin, and the patient noted significant improvement on arrival to the EmergencyDepartment.
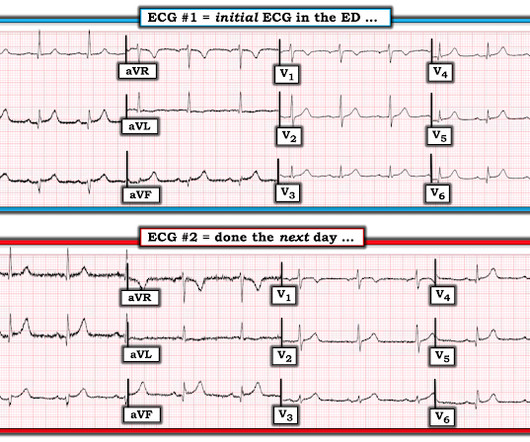
A 69 year old woman with a history of hypertension presented to the emergencydepartment by EMS for evaluation of chest pain and shortness of breath. A month later, she presented again to the emergencydepartment with a few hours of chest pain that resolved before ED presentation. This was written by Hans Helseth.
He presented to the emergencydepartment for evaluation. Patients with suspected ACS should be evaluated with echocardiography. This could have been another clue for facilitating earlier recognition of tihs patient's post-event pericarditis. How extensive was this patient's heart disease prior to this recent event?
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergencydepartment with chest pain. html ) Despite an undetectable troponin and three normal EKGs, the nature of the patients symptoms and his positive cardiac history warranted concern for ACS.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content