This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
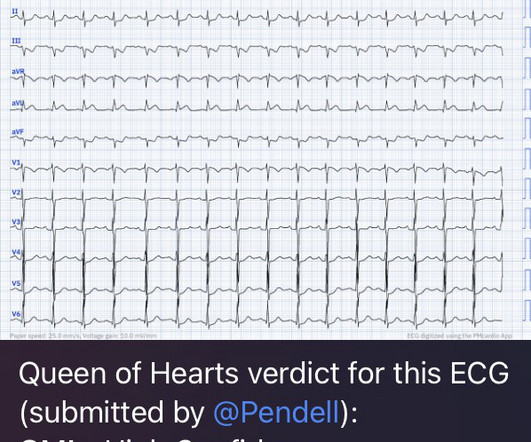
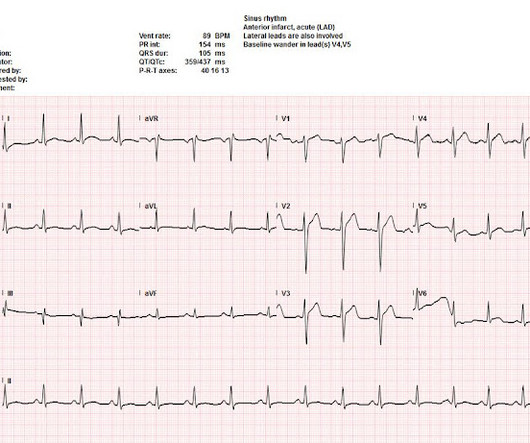
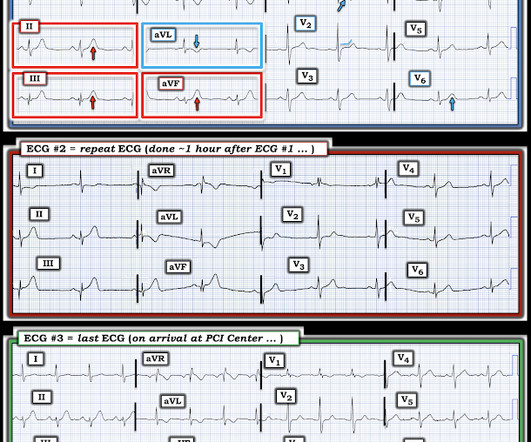
He presented to the EmergencyDepartment with a blood pressure of 111/66 and a pulse of 117. He was rushed by residents into our critical care room with a diagnosis of STEMI, and they handed me this ECG: There is sinus tachycardia with ST elevation in II, III, and aVF, as well as V4-V6. He had this ECG recorded.
Case 1: Case 2: Case 3: Triage ECGs labeled ‘normal’ There have been a number of small studies suggesting that triage ECGs labeled ‘normal’ are unlikely to have clinical significance, and therefore that emergency physicians should not be interrupted to interpret them, and that such patients can safely wait to be seen.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the EmergencyDepartment via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. looked at consecutive patients with PE, ACS, or neither. What do you think? ng/mL, BNP 2790, and lactate 3.7.
She arrives in the emergencydepartment (ED) with decreased level of consciousness and shock. Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients. She has a history of hypertension and non-insulin dependent diabetes mellitus.
The cardiologist recognized that there were EKG changes, but did not take the patient for emergent catheterization because the EKG was “not meeting criteria for STEMI”. Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? Annals of Emergency Medicine 2011; Suppl 58(4): S211. Murakami MM.
, tells us that we physicians do not need to even look at this ECG until the patient is placed in a room because the computer says it is normal: Validity of Computer-interpreted “Normal” and “Otherwise Normal” ECG in EmergencyDepartment Triage Patients I reviewed this article for a different journal and recommended rejection and it was rejected.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergencydepartment with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion.
He arrived in the emergencydepartment hemodynamically stable. ACS would be highly unusual in a young athlete, and given the information on his race bib, one must first suspect that the abnormal ST elevation is due to demand ischemia, not ACS. On his bib it stated that he had a congenital heart disorder.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). There is mixed overlap of ST-segment elevation (STE), ST-segment depression (STD), Hyperacute T waves (HATW), and deWinter pattern (which the ACC regards as a STEMI-equivalent but is better suited under the blanket of OMI).
Many conditions outside of acute coronary syndrome (ACS) mimic ST-elevation myocardial infarction (STEMI), but only a handful of cases have reported ST-elevations (STE) in the setting of pancreatic inflammation where underlying ACS was excluded. Mimics of ST elevation myocardial infarction (STEMI). Click to enlarge.)
Written by Bobby Nicholson What do you think of this “STEMI”? A man in his 90s with a history of HTN, CKD, COPD, and OSA presented to the emergencydepartment after being found unresponsive at home. Vital signs were within normal limits on arrival to the EmergencyDepartment. Blood glucose was not low at 162 mg/dL.
Written by Kaley El-Arab MD, edits by Pendell Meyers and Stephen Smith A 61-year-old male with hypertension and hyperlipidemia presented to the emergencydepartment for chest tightness radiating to the back of his neck that has been intermittent for the past day or two. It is true this ECG does not meet STEMI criteria (there is 1.0
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergencydepartment with 2 days of heavy substernal chest pain and nausea. The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Is there STEMI?
This was sent by anonymous The patient is a 55-year-old male who presented to the emergencydepartment after approximately 3 to 4 days of intermittent central boring chest pain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin. It is unknown when this pain recurred and became constant.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. Upon arrival to the emergencydepartment, a senior emergency physician looked at the ECG and said "Nothing too exciting." From Gue at al.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. His response: “subendocardial ischemia. Anything more on history? POCUS will be helpful.”
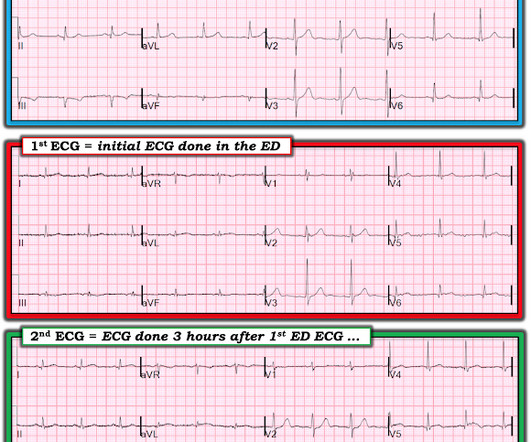
STEMI was activated and the patient went to Cath on arrival. Such aggressive investigation was particularly warranted in this case because of symptoms compatible with ACS, as well as an equally frightening revelation of family history. Conjecture aside, I believe the lesson here, ultimately, is serial ECG’s. link] [1] Mirand, D.
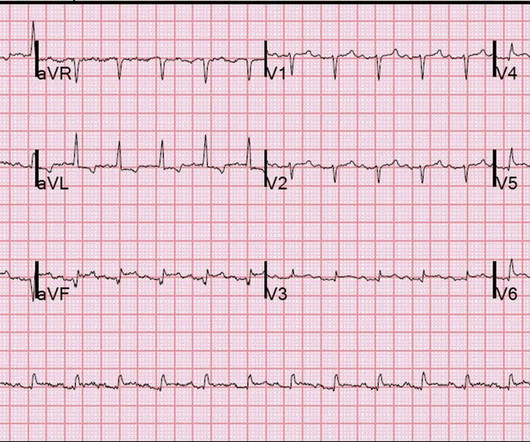
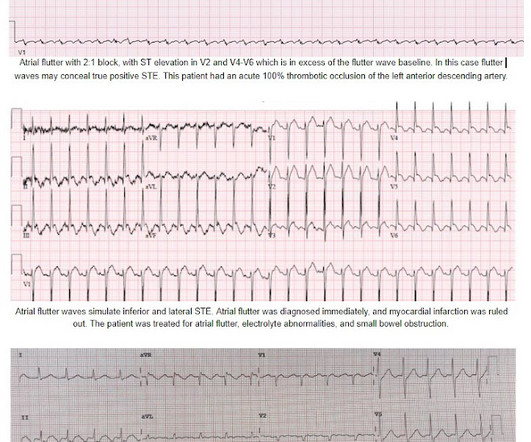
Is this inferor STEMI? Atrial Flutter with Inferior STEMI? Inferolateral ST elevation, vomiting, and elevated troponin The treating team did not identify the flutter waves and they became worried about possible "STEMI" (despite the unusual clinical scenario). The EM provider asked if the cardiologist thought it was a "STEMI."
Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Also note that they allow ST depression c/w posterior MI to be a STEMI equivalent. Kurkciyan et al.
STEMI , ST-segment elevation acute myocardial infarction ). 1 Initial diagnosis of STEMI ECG Management Recommendation Level of evidence A 12-lead ECG should be interpreted immediately (within 10 minutes) at first medical contact. I B Designated PCI centres should provide angiography and reperfusion 24/7 without delay.
A 35-year-old male presented to the emergencydepartment complaining of chest pain that started 1.5 5 Studies looking at this phenomenon in the emergencydepartment setting for patients presenting with chest pain are lacking. Dr. Young is an emergency physician at Saint Francis Hospital and Medical Center, Hartford, Conn.
But if they do present: The very common presentation of diffuse STD with reciprocal STE in aVR is NOT left main occlusion , though it might be due to sub total LM ACS, but is much more often due to non-ACS conditions, especially demand ischemia. All are, however, clearly massive STEMI. TIMI 0/1 flow).(61,62)
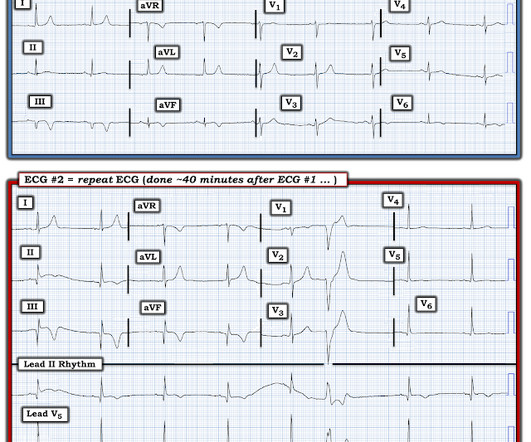
While in the emergencydepartment, he undergoes an additional ECG: 00:49 - Not much change Second ECG with measurements and calculations Magnified view of second ECGs measurements and calculation It is still "negative" for LAD occlusion (less than 23.4) Despite having acute coronary occlusion by cath, his ECGs never met STEMI criteria.
52-year-old lady presents to the EmergencyDepartment with 2 hours of chest pain, palpitations & SOB. These elevations meet STEMI criteria ( ≥ 1mm in 2 contiguous leads). In STEMI, they are generally upright and large in proportion to the QRS. So this argues against acute STEMI. This case is tough.
A man in his 60s with a history of severe alcohol use disorder and epidural abscess on long-term ciprofloxacin presented to the emergencydepartment after an episode of syncope while standing in line at a grocery store. Moreover, the Queen is only supposed to be used with a high pretest probability of ACS/OMI. Is it STEMI?
He had no symptoms of ACS. The remainder of his EmergencyDepartment stay was uneventful. The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? Physician interpretation: "No STEMI." Physician: "No STEMI."
I finished my residency of Emergency Medicine and I’m working at a great EmergencyDepartment here in Brazil. Since then, I started looking for OMI EKG findings and not just STEMI. mm in lead I, thus not STEMI criteria) and was finally understood by the cardiologist.
Because the patient's pain had resolved completely and cardiology had declined immediate intervention, the patient was admitted but continued to board in the emergencydepartment. Approximately 4 hours after arrival, the patient was re-examined by the emergency physician. There is no age cut-off for ACS. 1] Wereski, R.,
She was brought to the EmergencyDepartment and this ECG was recorded while she was still feeling nauseous but denied chest pain, shortness of breath, or other symptoms: What do you think? I wouldn't activate the lab for this EKG alone, but if the patient is clinically compatible with ACS you could call a heart alert.
The Smith-Modified Sgarbossa Criteria Accurately Diagnose Acute Coronary Occlusion in EmergencyDepartment Patients With Ventricular Paced Rhythm. And, in cases like the elderly patient with new-onset chest pain presented here — definitive diagnosis of acute STEMI is sometimes deceptively easy. Dodd1 , Deborah L.
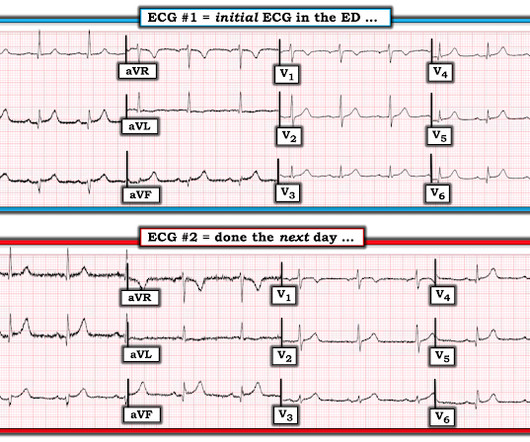
These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? Appropriately, the physicians repeated the ECG 20 minutes later and it was diagnostic of anterior STEMI. QTc is the computer measurement. 100% LAD occlusion.
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in EmergencyDepartment COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. 12 All STEMI patients had very high cTn typical of STEMI (cTnT > 1.0 of Cardiology AC, Others. Available from: [link] 9.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergencydepartment with substernal chest pain for 3 hours prior to arrival. The screening physician ordered an EKG and noted his ashen appearance and moderate distress. Triage EKG: What do you think?
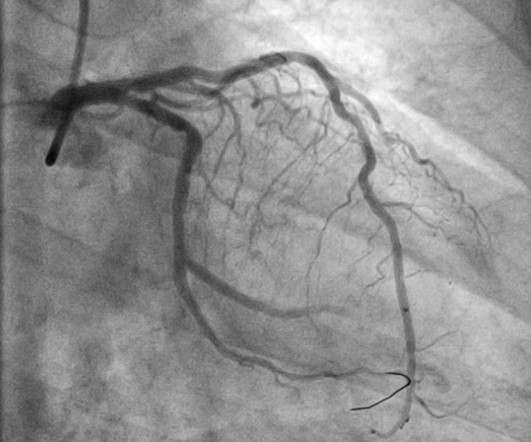
The clinicians later stated they had had no suspicion of ACS, but that the faculty wanted a troponin anyway. PCI mid LCx So this is an OMI (Occlusion Myocardial Infarction), but not a STEMI Echo: Decreased left ventricular systolic performance, mild/moderate. Angiogram: LM 30% ostial. distal stent patent. Sandoval Y. Murakami M.
STEMI negative : the EMS automated interpretation read, “STEMI negative. According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists. Sinus bradycardia.”
Case submitted and written by Dr. Mazen El-Baba and Dr. Emily Austin, with edits from Jesse McLaren A 50 year-old patient presented to the EmergencyDepartment with sudden onset chest pain that began 14-hours ago. This doesn’t meet STEMI criteria so in the current paradigm there’s no urgency to getting an angiogram.
Background: ST-segment elevation myocardial infarction (STEMI) is a critical condition requiring rapid diagnosis and intervention. While ECGs play a central role in detecting STEMI, misinterpretations often occur, leading to unnecessary catheterization or missed diagnoses. Paper: Lee SH, Jeon KL, Lee YJ, Ko YG, Choi D, Hong MK, et al.
The is very small STE in III and aVF which do not meet STEMI criteria, hyperacute T waves, reciprocal TWI in aVL, and maximal STD in V2-V3 showing posterior OMI. The ECG was transmitted to the Emergency Medicine physician who recognized inferior and posterior OMI findings, and confirmed that the patient has potential ACS symptoms.
She presented to the EmergencyDepartment at around 3.5 But thankfully, when the clinical context is clearly and highly concerning for ongoing ischemia from ACS, this distinction doesn't matter much. Final Diagnosis: "STEMI" (of course, as you can see in the ECGs above, this is not true, by definition this was NSTEMI.
His first EKG is shown below, with a lead II rhythm strip: EKG 1, 1645 A provisder who is looking for STEMI would not see much in this EKG. It is possible that the T waves in this EKG are of an intermediate morphology between full-blown STEMI and inferior reperfusion. This is the classic morphology of hyperacute T waves.
A 69 year old woman with a history of hypertension presented to the emergencydepartment by EMS for evaluation of chest pain and shortness of breath. Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. Truly, the Marquette 12 SL algorithm correctly identifies this STEMI.
He presented to the emergencydepartment for evaluation. 50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). Patients with suspected ACS should be evaluated with echocardiography.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content