This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The post JJ 16 Heparin for ACS and STEMI appeared first on Emergency Medicine Cases. Does heparin - LMWH or unfractionated heparin - benefit the patient with a pretty good story for angina with a bump in their troponin and some ST depression in the lateral leads? And for STEMI too. But should we? But should we?
David Didlake @DidlakeDW EMS personnel responded to the residence of an 81 y/o Male with syncope. Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates). His spouse had called 911 after she heard a loud “thud” in the adjacent room. Type I ischemia.
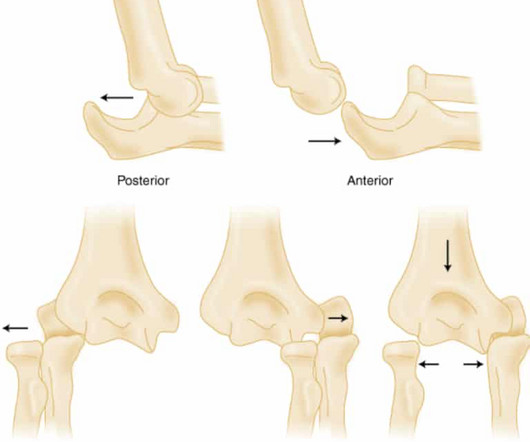
Elbow Dislocation Definition: Disarticulation of the proximal radius & ulna bones from the humerus Epidemiology: Incidence Second most common joint dislocation (after shoulder) in adults Most commonly dislocated joint in children Accounts for 10-25% of all injuries to the elbow ( Cohen 1998 ) Posterolateral is the most common type of dislocation (..)
Pediatric Buckle and Greenstick Forearm Fractures: Basics The junction of the metaphysis and diaphysis in pediatric long bones is an area of biomechanical transition (Light, 1984) Thin metaphyseal cortex meets the thick cortex of the diaphysis Or in Emergency Medicine terms, “ Thick bone meet thin bone.” J Bone Joint Surg Br. 2001;83:1173-5.
Case A patient arrives via EMS from the bus station complaining of fever, vomiting, and back pain. The biggest change has been the gradual replacement of diacetylmorphine (heroin) by fentanyl and other synthetic opioids. Their back has worsened significantly over the past 24 hours with radiation down the left leg.
What are the most useful historical factors to increase and decrease your pretest probability for ACS? Which cardiac risk factors have predictive value for ACS? Why should the words "troponitis" and "troponemia" be banned? How should high sensitivity troponin be interpreted differently than conventional troponin? and many more.
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. If the patient continues to have symptoms concerning for ACS, troponin testing should be pursued. SVT is not a presenting dysrhythmia consistent w/ ACS.
REBEL Cast Ep114 – High Flow O2, Suspected ACS, and Mortality? PMID: 33653685 Clinical Question: Is there an association between high flow supplementary oxygen and 30-day mortality in patients presenting with a suspected acute coronary syndrome (ACS)? Click here for Direct Download of the Podcast Paper: Stewart, RAH et al.
According to the EMS narrative, this patient initially refused hospital transport and advised that he would seek evaluation at a later time with his personal physician. He called 911, and EMS crews subsequently found him diaphoretic and vomiting. A 12 Lead ECG was recorded. It’s important to stress the presence of a normal QRS (i.e.,
EMS arrived and found him in Ventricular Fibrillation (VF). Then assume there is ACS. This patient was witnessed by bystanders to collapse. They started CPR. He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. After 1 mg of epinephrine they achieved ROSC. sodium bicarbonate.
We’ll keep it short, while you keep that EM brain sharp. A 68-year-old male with a past medical history of hypertension, diabetes mellitus, and coronary artery disease with a drug eluting stent placed 2 months ago presents with dizziness and vomiting that began 3 hours ago. Symptoms may range from days to months prior to stroke onset.
Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. The TOMAHAWK Investigators.
He presented to EMS with extreme pallor, Levine sign, diaphoresis, bilateral arm pain, and an apprehensive sense of doom. It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). ACE inhibitors, or potassium-sparing diuretics), are particularly susceptible.
RBBB + LAFB in the setting of ACS is very bad. Some patients have baseline RBBB with LAFB, but in patients with likely ACS, these are associated with severe infarction with cardiac arrest, cardiogenic shock or impending shock. Patients with ACS and RBBB/LAFB usually have a left main vs. proximal LAD. There is STE in aVR.
The post Hemolytic Uremic Syndrome (HUS): Rebaked Morsel appeared first on Pediatric EM Morsels. HUS is often associated with bloody diarrhea … but… There is a variant of HUS (D-) that is not associated with diarrhea; HUS (D-) does not have seasonal variation and is relatively uncommon. 2021 May;232:200-206.e4. 2020.12.077.
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS. looked at consecutive patients with PE, ACS, or neither.
He reported to EMS a medical history of GERD only. V2 – in the final EMS ECG the ST segment was baseline. V3 – in the final EMS ECG the ST segment was still slightly depressed. The physical exam was unremarkable for diaphoresis or pallor, and he denied any episodes of vomiting. However, in this context (i.e. ST-elevation, etc.)
VS abnormalities can drive this as well Strongly consider reversal of AC (this will typically come after control) Stopping the Bleeding PPE: these things bleed like stink. REBEL EM: Do Patients with Posterior Epistaxis Managed by Posterior Packs Require ICU Admission? This will be pretty location specific.
Written by Pendell Meyers A man in his 40s called EMS for acute chest pain that awoke him from sleep, along with nausea and shortness of breath. Because the most severe LAD OMIs can cause ischemic failure of the RBB and LAF, any patient with ACS symptoms and new RBBB and LAFB with any concordant STE has LAD OMI until proven otherwise.
The patient is an adult male with a gunshot wound to the chest, and they’re combative with emergency medical services (EMS). According to a recent study in the Journal of Surgical Research [3] , 44% of all penetrating thoracic trauma patients presented to a non-trauma center (not a level 1 or level 2 ACS defined trauma center).
He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic. Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? Smith comment 2: I frequently see failure to control BP in patients with acute chest pain or acute heart failure. Smith: What???!!!
PARAMEDIC 3 randomized 6,000 (but they were supposed to get to 15,000) patients with out of hospital arrest from multiple EMS agencies in the UK to either an IO or IV to start. This month we cover a few out-of-hospital arrest trials. More PECARN goodness and we answer the question: are ants better doctors than human doctors? N Engl J Med.
This should prompt immediate investigation into supply-demand mismatching, or ACS. There is bradycardic Atrial Fibrillation with broad ST-depression in most leads and perceptible ST-elevation in aVR. But there’s some peculiar features about this ECG: The unusually short QT The “scooped out” appearance of the ST-segments.
Reference: EM@3AM – Heat Stroke Case 2: 40-year-0ld female feels unwell but no other specific complaints. Reference: Reyner K, Heffner AC, Karvetski CH. Complete primary and secondary survey. Start cooling as quickly as you can, and stop at 102. Resuscitate and administer antibiotics. ROS unremarkable. Am J Emerg Med.
A study published by Cambridge University Press examined patient outcomes over a decade during which Emergency Medical Service (EMS) systems decreased backboard use as they transitioned from SI to SMR protocols. However, recent research has called this practice into question. to prevent movement of the spine.
Notoriously elusive, with a high misdiagnosis rate, thoracic aortic dissection (AD) can mimic many conditions, including acute coronary syndrome (ACS, the most common), gastroesophageal reflux disease (GERD), stroke, and spinal-cord compression. The patient is admitted for ACS to a cardiologist who says he will see the patient in the morning.
She took an oxycodone and called EMS. The patient was thought to have low likelihood of ACS, and cardiology recommended repeat troponin, urine drug testing, and echocardiogram. At that point, cardiology elected to treat for ACS. Written by Willy Frick A 40 year old woman was at home cooking when she developed chest pain.
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. Smith : This is ACS even if the troponin returns normal, and the first troponin especially might return normal. This results in Type I MI. This results in Type II MI. Severe HTN d.
As Smith and Meyers explained in a 2020 article in EM News : “What should we do in the meantime while we are still stuck in the STEMI paradigm in daily practice? Most importantly, while waiting for the paradigm to evolve, maintain focus on our true goal for our patients with ACS: to identify and reperfuse patients with acute occlusion MI.”
Click here for Direct Download of the Podcast Paper: Aykan AC et al. Because the lungs receive 100% of cardiac output, it has been hypothesized that a lower dose of thrombolytic therapy may still be effective with a better safety profile [3][4]. REBEL Cast Ep123: Reduced-Dose Systemic Peripheral Alteplase in Massive PE?
EMS obtained the following vital signs: pulse 50, respiratory rate 16, blood pressure 96/49. It appears EMS obtained two EKGs, but unfortunately these were not saved in the medical record. The EMS crew was only BLS certified, so EKG interpretation is not within their scope of practice. Before and after of the LAD shown below.
Simulation allows EMS clinicians to train for scenarios they may encounter in the field. Depending on the EMS providers, these scenarios may be ones that they have already encountered or those that they have yet to see in real life. This was a real issue because all our friends lived down and across the street.
The SGEM bottom line was there is moderate level of evidence that ACS can be excluded in adult patients with recurrent, low-risk chest pain using a single hs-troponin below a validated threshold without further diagnostic testing in patients who have a CCTA within the past two years showing no coronary stenosis. His vital signs are normal.
Article: Vaeli Zadeh A, Wong A, Crawford AC, Collado E, Larned JM. References: Vaeli Zadeh A, Wong A, Crawford AC, Collado E, Larned JM. Rezaie, MD (Twitter/X: @srrezaie ) The post Congestive Heart Failure and Sepsis: A Closer Look at Fluid Management appeared first on REBEL EM - Emergency Medicine Blog. 2.89, p = 0.01.
EMS finds him supine, alert and oriented, and without any gross distress. In isolation, however, syncope does not hold significant weight for OMI – as opposed to something like crushing chest discomfort, for example – although stereotypical ACS might become blurry in both the elderly and diabetic populations.
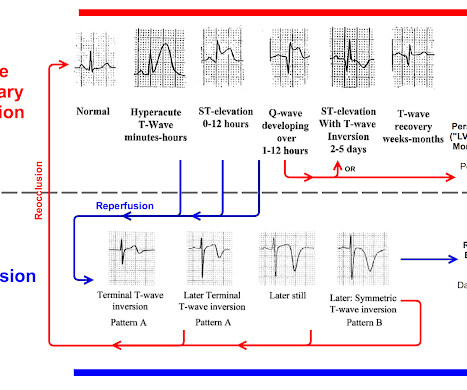
You must understand this and the dynamic nature of ACS to provide excellent care for such patients. Here is the OMI progression of ECG findings for review: You can see that OMI ECG findings must "deflate" and pass through normal or near-normal in order to get to reperfusion findings. This is termed " pseudo-normalization."
About 2 hours later the patient arrived at a PCI-capable center and repeat ECG was obtained: The transferring EMS crew noted “runs of VT” during transport. Similarly, the OMI paradigm respects ACS as a dynamic process in which ECG changes reflect the phase of myocardial injury and risk stratify which patients may benefit from emergent PCI.
EMS arrived — and recorded 2 ECGs. The emergency physician was skeptical and believed the ECG to be a mimic, a false positive. So they looked into the patient's chart. Learning Point: 1. If you have old ECGs available, seek them out and compare today's ECGs to those old one. That is coming in the future with further training.
References: Ross RK, Kinlaw AC, Herzog MM, Funk MJ, Gerber JS. When you read the Morsel on Perichonditis of the ear last week ( or perhaps the Plantar Puncture Morsel from many many many weeks ago ) you may have objected because of the mention that, when indicated, fluroquinolones are safe in children. Which is a risk of 1 event for 62.5
I was there and said, "No, I think this is all due to severe chronic cardiomyopathy and cardiac arrest due to primary ventricular fibrillation, not due to ACS." _ Why did I say that? Patient received 11 shocks by ICD and was in V-fib when EMS arrived. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines.
With EMS, patient had a GCS of 3 and was saturating 60% on room air. He improved to 100% with the addition of non-rebreather, however remained altered and was intubated by EMS with ketamine and succinylcholine. Vital signs were within normal limits on arrival to the Emergency Department. or basilar ischemia. Version 2 = 0.0272.
ACS surgeons appeared to select surgery as their initial choice substantially more frequently than other subspecialties. ACS surgeons would have sent 6/43 patients for ERCP or MRCP (14%), whereas surgical oncologists would have sent a higher percentage of patients for ERCP or MRCP (7/18 or 38.9%). and specificity of 88.0%
Today’s pain lasted around 20 mins, but was severe enough that the patient called EMS. Pain largely resolved prior to EMS arrival but completely subsided after prehospital NTG and aspirin. There is no age cut-off for ACS. At the time of arrival to the ED, the patient reported 1/10 chest pain with normal vital signs.
Welcome back to the “52 in 52” series. This collection of posts features recently published must-know articles. Today we look at the CENSER trial. vs 48.4% (OR 3.4, 5.53) Takeaways: Positive trial => there was a statistically significant rate of shock control attained with the treatment arm. vs 48.4% (OR 3.4,
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content