This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Today on the emDOCs cast with Brit Long ( @long_brit) , we cover immune checkpoint inhibitors and adverse events. The post emDOCs Podcast Episode 113: Immune Checkpoint Inhibitor Adverse Events appeared first on emDOCs.net - Emergency Medicine Education. Immune checkpoint inhibitors: An emergency medicine focused review.
He denied any specific prodrome of gross palpitations, however did endorse feeling quite dizzy just before the event. Given no clinical prelude of anginal (or equivalent) descriptors, prior to the acute event, risk stratification of the ECG and Troponin was pursued via Echo and nuclear Myocardial Perfusion Imaging (MPI).
Furthermore, if this occurs at all, it is a rare event. It is not small but rather large plaques, which may not be producing significant stenosis, that undergo rupture with acute occlusive thrombosis, resulting in myocardial infarction and other ischemic events. years, with the interval as long as 12 or 18 years in some studies.
The biggest change has been the gradual replacement of diacetylmorphine (heroin) by fentanyl and other synthetic opioids. Along the same time, a veterinary sedative, xylazine , became popular in Puerto Rico in individuals who used injection drugs [3]. We treat with wound care and reserve surgical management only for limbs that are no longer viable.
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. There are other reasons aside from ACO for troponin elevations: Type 1: MI due to a spontaneous coronary atherosclerotic event. Send the troponin just to make sure.
Myth 1 Absence of Classic Chest Pain obviates the need for ACS work up The absence of chest pain in no way excludes the diagnosis of ACS. Around 33-50% of the patients with ACS present to the hospital without chest pain. Close to 20% of patients diagnosed with acute MI present with symptoms other than chest pain.
Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? If we thought about ACS, we brought them in. Date: June 30th, 2022 Reference: McGinnis et al. AEM June 2022. AEM June 2022.
Myth #1: Musculoskeletal Adverse Events (MAE) This concern is likely the most common reason fluoroquinolones are rarely used in children. Musculoskeletal Adverse Events include: Articular cartilage damage causing arthralgias or arthritis , Tendonitis , and Tendon rupture. Which is a risk of 1 event for 62.5
The faculty physician thought this is highly likely to be ACS. I do not think it is possible for a 2nd trop to remain undetectable in a patient then goes on to rule in for acute MI, unless there is a 2nd event. I know of no data on unstable angina/30-day adverse events/acute MI after 2 serial undetectable trops.
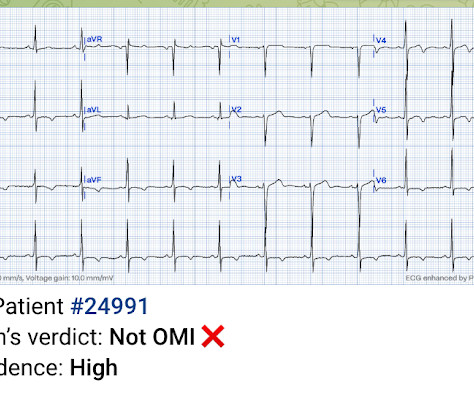
A healthy 45-year-old female presented with chest pain, with normal vitals. The computer interpretation was “ST elevation, consider early repolarization, pericarditis or injury.” What do you think? There’s normal sinus rhythm, normal conduction, borderline right axis, and normal voltages. There’s TWI in aVL but this is concordant to its QRS.
Smith : As Willy states, ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). Smith : As Willy states, ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). So I would be worried about inferior OMI. At midnight.
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Even in patients whose moderate stenosis undergoes thrombosis, most angiograms show greater than 50% stenosis after the event.
Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? If you are worried about aortic dissection, you also want the BP to be lowered, though you would do it first with esmolol to decrease the dP/dT (change in pressure over change in time). The ST depressions in I and aVL have resolved. Probably the latter.
VS abnormalities can drive this as well Strongly consider reversal of AC (this will typically come after control) Stopping the Bleeding PPE: these things bleed like stink. Take Home Points: Posterior epistaxis is a rare, life-threatning presentation. Literature doesn’t defend this approach but, the lit is pretty sparse.
The device could be very useful fo screening large numbers of people prior to access to an indoor event, for instance, or in community clinics to quickly determine if people are infected. However, if we are to learn the lessons of the pandemic, we need to develop strategies that will assist us with the next one.
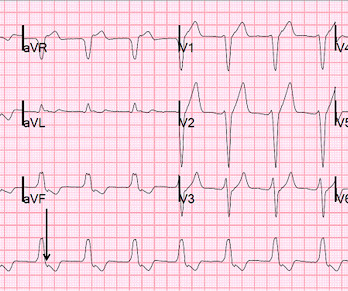
Because the most severe LAD OMIs can cause ischemic failure of the RBB and LAF, any patient with ACS symptoms and new RBBB and LAFB with any concordant STE has LAD OMI until proven otherwise. Even before looking at the initial ECG — this patient is in a high prevalence group for having an acute event. Long term outcome is unavailable.
Because there was proven thrombus (ACS) but the troponin never went above the 99% reference range (and therefore cannot be called MI -- definition of MI requires rise and/or fall of troponin with at least one value above the 99% reference range), this is UNSTABLE ANGINA with ST Elevation. Fortunately, that is exactly what happened.
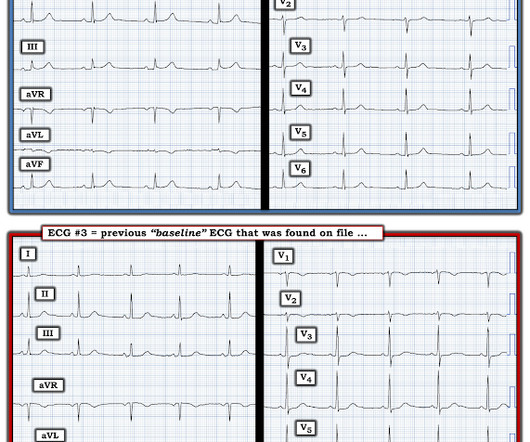
link] = My Comment by K EN G RAUER, MD ( 11/14 /2023 ): = One of the most helpful clinical clues in support that an acute cardiac event is ongoing — is the finding of " dynamic " ECG changes. The emergency physician was skeptical and believed the ECG to be a mimic, a false positive. So they looked into the patient's chart. Learning Point: 1.
Click here for Direct Download of the Podcast Paper: Aykan AC et al. Because the lungs receive 100% of cardiac output, it has been hypothesized that a lower dose of thrombolytic therapy may still be effective with a better safety profile [3][4]. REBEL Cast Ep123: Reduced-Dose Systemic Peripheral Alteplase in Massive PE?
3) RV Failure leads to hypotension but NOT pulmonary edema (unlike LV failure) 4) Repeat ECGs, right sided ECG and bedside echo may be helpful in making a diagnosis of ACS. As a result — the onset of any acute event that may have occurred is uncertain. Any cause of pulmonary hypertension.
The patient was thought to have low likelihood of ACS, and cardiology recommended repeat troponin, urine drug testing, and echocardiogram. At that point, cardiology elected to treat for ACS. Initial hscTnI was 10 ng/L (ref. <14). There was no recommendation for repeat ECG. Angiography is shown below.
Thus, these troponins are very concerning for ACS, and subsequent ones will probably be diagnostic of acute MI. Smith comment: No patient over 25 years of age with unexplained chest burning should be discharged without a troponin rule out, no matter how normal the ECG. His angiogram is shown below. Heitner et al.
This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. But I'd be less certain about an acute event without more information and prior and/or serial tracings. He reports feeling nauseated with emesis. He denies taking aspirin or antihypertensive medications for the last year and a half.
No wall motion abnormality This shows that significant ACS can have ZERO WMA!! There are also subtly hyperacute T-wave in I, aVL, and V2-V6. There is also a very negative (reciprocally inverted) T-wave in lead III, and a down-up T-wave in aVF, both of which are highly suggestive of occlusion of the LAD or D1. The S-wave is reconstituted.
I was there and said, "No, I think this is all due to severe chronic cardiomyopathy and cardiac arrest due to primary ventricular fibrillation, not due to ACS." _ Why did I say that? For this reason we did not believe this was an acute coronary event and did not activate the cath lab. Here is the initial ED ECG. What do you think?
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Link to abstract Link to full text 2) Use of Morphine in Non-STE-ACS is independently associated with mortality, at odds ratio of 1.4
But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Potassium was normal.
He had no symptoms of ACS. His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS." A troponin this high in a patient with no known chronic troponin elevation, and active acute ACS symptoms, has a very high likelihood of type 1 ACS regardless of the ECG.
There were zero patients in this study with a "normal" ECG who had any kind of ACS! This defies all previous data on acute MI which would show that even undetectable troponins do not have a 100% negative predictive value. So this study is actually worthless. Deutch et al. West J Emerg Med 2024).
which would suggest reduced rates of major adverse cardiac events with coronary artery bypass grafting." He had been smoking an opiate and suddenly collapsed. He was ventilated with BVM on arrival. He awoke with naloxone. This EKG was recorded as part of a standing order for critical care. He denied any CP or SOB. It does not radiate.
But it still doesn’t meet STEMI criteria, so the patient was referred to cardiology as ACS. Are there any signs of occlusion or reperfusion? There’s normal sinus rhythm, normal conduction, normal axis, normal R wave progression and normal voltages.
Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion. Whether this represents a potential acute cardiac event would depend on the history, comparison with prior tracings and serial tracings. He denied any chest discomfort, or difficulty breathing.
Moreover, the Queen is only supposed to be used with a high pretest probability of ACS/OMI. QTc/QUc is in the range of 630 msec. What is the most likely cause of the patient’s ECG findings, and what would be your first step in management? We just finished training version 2 with some cases of hypokalemia, so that is in the future.
The trade off to using FI for these challenging airways is the consideration of an aspiration event, the initial indication for RSI. First pass success (FPS) is key as increased attempts correlate to increased desaturation (>10%) events (~10% on first attempt, ~30% on second attempt, ~60% for 4+ attempts) (15).
In our opinion it should not be given in ACS unless you are committed to the cath lab. Learning Point: Any NSTEMI patient with active ongoing ACS symptoms refractory to medical management is supposed to go to the cath lab within 2 hours if available, per all guidelines in world, regardless of ECG findings. He was diagnosed as NSTEMI.
The AHA/ACC guidelines recommend emergent cardiac catheterization for patients with concern for ACS and refractory chest pain despite maximum medical therapy defined as aspirin + clopidogrel/ticagrelor + heparin/enoxaparin. link] He was admitted to the cardiology unit for serial troponin measurements and concern for possible ACS.
SCAD isn’t rare, especially in women Historically SCAD had been identified in 22% of ACS cases in women. Pregnancy is not a common cause of SCAD When ACS occurs in the peripartum period, SCAD is responsible in 43% of cases. This rate and height of troponin rise strongly suggested a type 1 MI. This case occurred 10+ years ago.
In addition to the small size of the ECG complexes on this tracing — I did not think the ECG features of an acute event were at all obvious. Prior episodes had simply resolved after brief symptoms, but the current episode had lasted for 2 hours without improvement, so she presented to the ED. No diaphoresis or vomiting.
No obvious adverse events were attributed to the thrombolytics. Second, the increased demand created by extreme tachycardia may exceed the ability of the coronary arteries to supply sufficient blood (due to preexisting three vessel or left main disease, with or without ACS). Christmas Eve Special Gift!! Serial troponins were negative.
A 90 yo with a history of orthostatic hypotension had a near syncopal event followed by chest pain. Chest pain and possible ischemia were attributed not to ACS, but to transient hypoperfusion from orthostatic hypotension. Chest pain was resolved upon arrival in the ED. His previous ECG was normal. What is it? Answer below.
The app also states that there is "suspected" ACS without ST elevation (NSTEMI), posterior fascicular block, sinus bradycardia, and LVH) Note on version 1 of the Queen: she will diagnose "OMI" whether it is an active or reperfused OMI. Translation from French: Acute Occlusion Myocardial Infarction with High Confidence.
titled “Intubation Practices and Adverse Peri-intubation Events in Critically Ill Patients from 29 Countries,” at least one major critical event occurred after intubation in 45.2% Up to 44% per other sources [12]. And according to a paper from Russotto et al. Of note, in the paper by Russotto et al.,
It is easy to say this in retrospect, especially not being the one in charge of this overcrowded waiting room full of unseen patients, but an elderly patient with known CAD and ongoing ACS-sounding chest pain despite medical management with positive troponin is already an indication for emergent cath, regardless of the ECG!
ED treatment should focus on airway, breathing, and circulation with consideration for cervical spine protection depending on the circumstances surrounding the event. One question that is commonly raised is whether these patients should be trauma activations. 4 Another study cited only 2.3
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content