This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Because the most severe LAD OMIs can cause ischemic failure of the RBB and LAF, any patient with ACS symptoms and new RBBB and LAFB with any concordant STE has LAD OMI until proven otherwise. There is no recognition of STEMI equivalency in this setting in the USA guidelines currently. Long term outcome is unavailable.
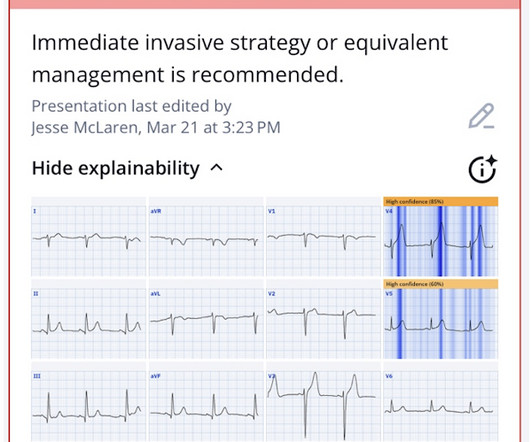
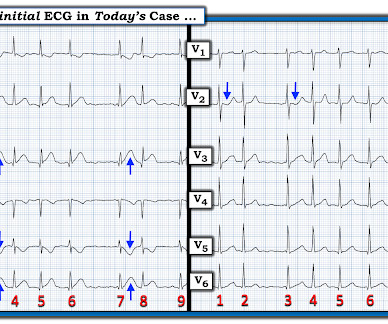
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. But there are also hyperacute T waves (HATW) in V4-5, which exclude early repolarization and pericarditis, leaving only LAD occlusion for this patient presenting with classic symptoms of ACS.
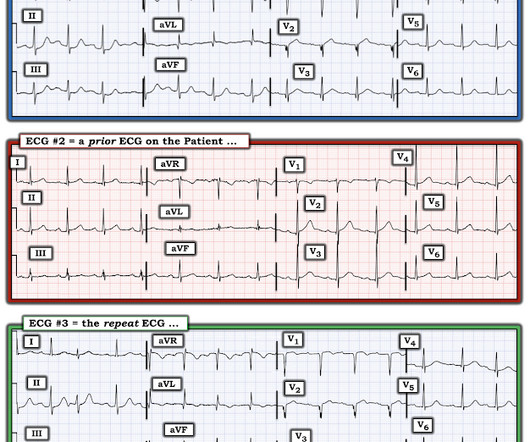
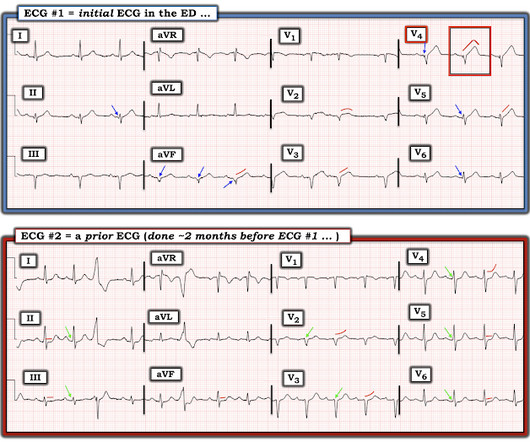
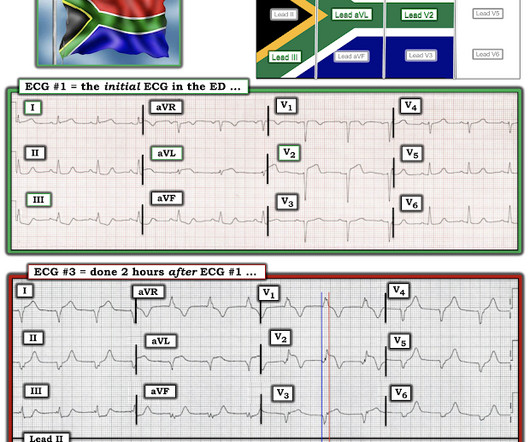
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. Furthermore, if this occurs at all, it is a rare event. He does have a recently diagnosed PE, and has not been taking his anticoagulation due to cost. He had a previous ECG on file: Proving the findings are new The cath lab was activated.
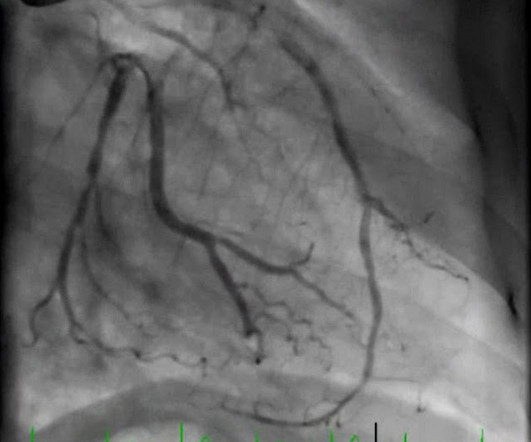
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Even in patients whose moderate stenosis undergoes thrombosis, most angiograms show greater than 50% stenosis after the event. From Gue at al.
The cardiologist recognized that there were EKG changes, but did not take the patient for emergent catheterization because the EKG was “not meeting criteria for STEMI”. Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? Assuming that was indeed a culprit, then this was ACS.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Smith : As Willy states, ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC).
There were zero patients in this study with a "normal" ECG who had any kind of ACS! So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. Deutch et al.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. This is not unusual. Take home 1.
Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Day 12 ECG: FINAL DIAGNOSIS: "NSTEMI" Despite the fact that his day 4 ECG easily meets STEMI criteria, the patient is diagnosed as NSTEMI. No TIMI flow was listed in the report. Am Heart J.
He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. Sensitivity was 87% for OMI in our validation study (it was 34% for STEMI criteria). So it can miss some OMI.
This patient could have very easily been overlooked, both because the ECG was STEMI negative and because the Q waves were attributed to an “old infarct”. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion. OMI or STEMI? As cardiology documented, “possible STEMI.
Troponin T peaked at 2074 ng/L (very high, typical of OMI/STEMI). 3) RV Failure leads to hypotension but NOT pulmonary edema (unlike LV failure) 4) Repeat ECGs, right sided ECG and bedside echo may be helpful in making a diagnosis of ACS. As a result — the onset of any acute event that may have occurred is uncertain.
Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. No wall motion abnormality This shows that significant ACS can have ZERO WMA!! Is it normal STE? This is a "Transient OMI".
Thus, these troponins are very concerning for ACS, and subsequent ones will probably be diagnostic of acute MI. For this test it is VERY low (very good) at 4% at the 99th percentile -- 26 ng/L, but it will not be so good at a level of 9 ng/L. Thus, one considers a test result that varies by 2 or less to be the same result. of the time.
Because there was proven thrombus (ACS) but the troponin never went above the 99% reference range (and therefore cannot be called MI -- definition of MI requires rise and/or fall of troponin with at least one value above the 99% reference range), this is UNSTABLE ANGINA with ST Elevation. This is not the case.
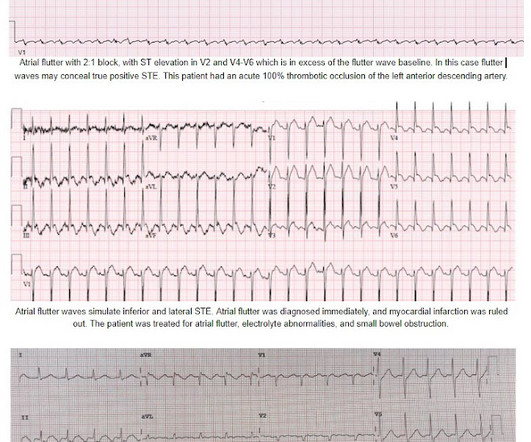
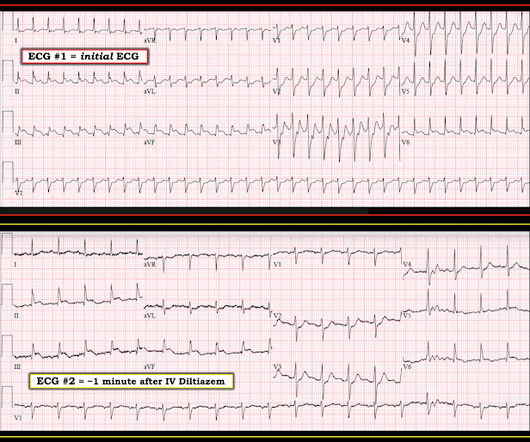
Is this inferor STEMI? Atrial Flutter with Inferior STEMI? Inferolateral ST elevation, vomiting, and elevated troponin The treating team did not identify the flutter waves and they became worried about possible "STEMI" (despite the unusual clinical scenario). The EM provider asked if the cardiologist thought it was a "STEMI."
This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. These include: i ) appreciation of how problematic the definition of “acute STEMI” can be; and , ii ) illustration of how dependence on this definition may result in overlooking acute coronary occlusion. Mokhtari et al. JACC 2016;67:1531.
The emergency physician asked the advice of Dr. Reiters because of absence of STEMI criteria. The app also states that there is "suspected" ACS without ST elevation (NSTEMI), posterior fascicular block, sinus bradycardia, and LVH) Note on version 1 of the Queen: she will diagnose "OMI" whether it is an active or reperfused OMI.
Only very slight STE which does not meet STEMI criteria at this time. I am immediately worried that this OMI will not be understood, for many reasons including lack of sufficient STE for STEMI criteria, as well as the common misunderstanding of "no reciprocal findings" which is very common with this particular pattern.
Discharge ECG showed antero-inferior reperfusion T wave inversion: Had the initial ECG been signed off as “STEMI negative” the patient could have arrested in the waiting room, with a poor cardiac and neurological outcome. First trop was 90 ng/L (normal <16 in females) and peak was 7,400 ng/L.
STEMI , ST-segment elevation acute myocardial infarction ). 1 Initial diagnosis of STEMI ECG Management Recommendation Level of evidence A 12-lead ECG should be interpreted immediately (within 10 minutes) at first medical contact. I C If possible, patients should bypass non-PCI centres to a PCI-capable centre.
The AHA/ACC guidelines recommend emergent cardiac catheterization for patients with concern for ACS and refractory chest pain despite maximum medical therapy defined as aspirin + clopidogrel/ticagrelor + heparin/enoxaparin. link] He was admitted to the cardiology unit for serial troponin measurements and concern for possible ACS.
The cardiologists decided to overrule the STEMI criteria and the cath lab activation was NOT cancelled, and she was taken immediately to the cath lab and found to have an acute thrombotic distal LAD occlusion (TIMI 0). At triage she stated her pain is still persistent, but it is mildly improved compared to when she decided to come to the ED.
Figure 1-1 My colleague, a faithful student of ECG interpretation, handed me the tracing and said that it warranted STEMI activation because of apparent terminal QRS distortion (TQRSD) in V2. Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. Takotsubo is a sudden event, not one with crescendo angina. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chest pain.
SCAD isn’t rare, especially in women Historically SCAD had been identified in 22% of ACS cases in women. A recent study found that SCAD causes almost 20% of STEMI in young women. Pregnancy is not a common cause of SCAD When ACS occurs in the peripartum period, SCAD is responsible in 43% of cases. A study by Hassan et al.
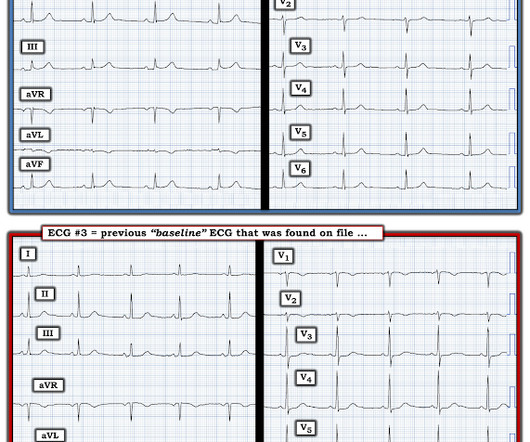
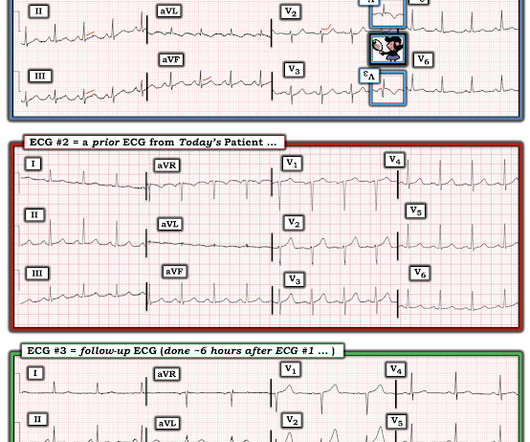
There is a very small amount of STE in some of the anterior, lateral, and inferior leads which do NOT meet STEMI criteria. One must always be careful when looking for "baseline" ECGs, because the prior ECG on file may have been during another ACSevent, as this one clearly was. This ECG is highly suspicious for LAD OMI.
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). In our opinion it should not be given in ACS unless you are committed to the cath lab. Unfortunately — 1.5
The patient has heart failure as a result of this event. If it is maximal in V1-V4, and the patient's presentation in consistent with ACS (as this certainly is), then it is DIAGNOSTIC of Occlusion with 90% specificity (We have an upcoming article that proves this). Angiogram: "ACS - Non ST Elevation Myocardial Infarction.
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
There’s mild inferior ST elevation in III that doesn’t meet STEMI criteria, but it’s associated with ST depression in aVL and V2 that makes it diagnostic of infero-posterior Occlusion MI (from either RCA or circumflex)– accompanied by inferior Q waves of unknown age. Are there any signs of occlusion or reperfusion?
The triage ECG was interpreted correctly as "No STEMI." This finally prompted a repeat ECG at 1341: 1350: Obviously STEMI(+) OMI. Obvious ACS history with ongoing pain despite medical management and upgoing troponin is an indication for emergent cath regardless of ECG findings. = The second troponin returned higher at 45 ng/L.
A 90 yo with a history of orthostatic hypotension had a near syncopal event followed by chest pain. In other words, after reperfusion therapy for STEMI, the appearance of AIVR is usually a good sign, meaning that the artery is reperfused. Chest pain was resolved upon arrival in the ED. His previous ECG was normal. What is it?
This morphology can be cause by or associated with cocaine: A Patient with Cocaine Chest Pain and Prehospital Computer interpretation of STEMI This is OMI of the anterior, lateral, and inferior walls until proven otherwise. But it does not meet STEMI criteria and it was not initially recognized. The cath lab was now activated.
Moreover, the Queen is only supposed to be used with a high pretest probability of ACS/OMI. Is it STEMI? We just finished training version 2 with some cases of hypokalemia, so that is in the future. The patient’s VBG resulted as I was speaking with him and confirmed my suspicions, showing a potassium of 1.6 What is going on here?
Since then, I started looking for OMI EKG findings and not just STEMI. Remember: these findings above are included as STEMI equivalent findings in the 2022 ACC Expert Consensus Decision Pathway on ACS Patients in the ED. mm in lead I, thus not STEMI criteria) and was finally understood by the cardiologist.
Guidelines say that if a patient has ACS but refractory pain, the patient should go emergently to the cath lab. Notice that much of the dark blue is concentrated on the QRS (R-wave); the QRS is totally ignored in the STEMI paradigm!! Fluids and morphine had been given and the patient had spontaneously converted to sinus rhythm.
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion).
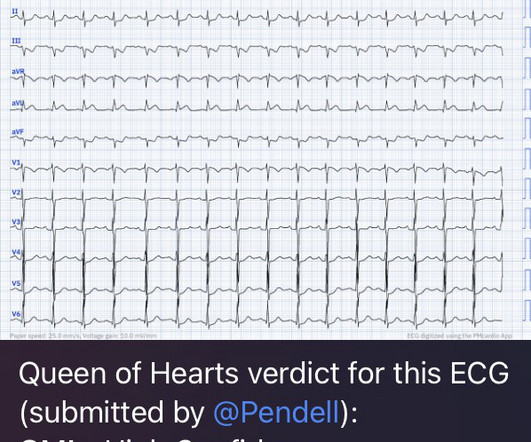
He had no symptoms of ACS. The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS." Physician: "No STEMI."
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. This case represents the same physiologic event as OMI in terms of the result on the myocardium, therefore with identical ECG features, however there may not be ACS!
Considering hyperacute T-waves have been accepted as STEMI equivalents, it is possible that pseudonormalization could gain more recognition as an indicator of ACS. Sequence of events in angina at rest: Primary reduction in coronary flow. References Noble RJ, Rothbaum DA, Knoebel SB, McHenry PL, Anderson GJ. Arch Intern Med.
Corroborating this is the subtle ST depression in V2-V3 which is inappropriate for the normal QRS complex, and in the context of ACS, we have shown this is quite specific for posterior OMI. In the context of ACS, ST depression maximal in V1-V4 (rather than V5-V6) not due to a QRS abnormality is specific for posterior OMI.
Could this be Septal STEMI (STE in V1 and aVR, with reciprocal ST depression in V4-V6?), In Septal STEMI , transmural ischemia of the septum is recorded by the overlying lead V1 as ST Elevation. Lead III is also on the right and might manifest ST Elevation in Septal STEMI. with ADDED STE in III?
These findings are very subtle but suspicious for LAD occlusion, as we have seen in many similar (but less difficult) cases on this blog: A man in his sixties with chest pain at midnight with undetectable troponin How long would you like to wait for your Occlusion MI to show a STEMI? Learning Points: Not all OMI will present as STEMIs.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content