This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Welcome to the first episode of the Broomedocs podcast for 2025. Justin and I are back for more nerdy goodness to make you smarter in the Resus room, or at a pub trivia night more likley… wether it is about salt correction, dissection or infection we can help you out! Listen in and learn! Dimer is useful in the low risk group. Emerg Med J.
VS abnormalities can drive this as well Strongly consider reversal of AC (this will typically come after control) Stopping the Bleeding PPE: these things bleed like stink. The idea behind abx is to prevent things like AOM and TSS but neither should be much of an issue with short term placement ICU Admission?
The patient was upgraded to the ICU for closer monitoring. showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS. looked at consecutive patients with PE, ACS, or neither. In fact, Kosuge et al. Stein et al. Kosuge et al.
Article: Vaeli Zadeh A, Wong A, Crawford AC, Collado E, Larned JM. Secondary Outcomes: Delayed hypotension, increased ICU stay, and other relevant outcomes. Utilized Egger’s linear regression and Begg and Mazumdar’s rank correlation test to assess publication bias. Studies without a clear timeframe for fluid administration.
Removed from cooling at 102 and admitted to ICU. Reference: Reyner K, Heffner AC, Karvetski CH. Cooling blanket placed, but temperature increases to 107F. Immersion cooling completed with ice between body bags. Temperature starts to decrease. Must consider differential in complex cases. Get consultants involved early. Am J Emerg Med.
Moreover, the Queen is only supposed to be used with a high pretest probability of ACS/OMI. The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course. QTc/QUc is in the range of 630 msec. Magnesium later resulted at 0.8 mg/dL, and ionized calcium was 0.73
Type 1 is the acute deterioration in kidney function seen in cardiogenic shock from ACS. It is important to realise that a referral to ICU for refractory cardiorenal syndrome may simply be a sign that the patient is reaching end of life. Type 1 is the acute deterioration in kidney function seen in cardiogenic shock from ACS.
Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Cardioversion will address the rhythm problem immediately, also if the chest discomfort subsides when SR is restored, ischemia from ACS becomes much less likely. In either case, prompt cardioversion is indicated.
In ICUs where advanced cerebral monitoring is not in routine use, target an MAP >80 mm Hg unless there are clinical concerns or evidence of adverse consequences (82.6%, 19/23). In ICUs where noninvasive monitoring of cerebral autoregulation is in routine use, maintain MAP at or near the predicted MAPOPT (88.2%, 15/17).
They found NO difference in drain failure rates ( 11% pigtail vs 13% chest tube P=0.74), total daily volume drained or length of ICU stay between groups. You ask your anaesthetist to get ready to sedate or intubate depending on their status – Significant risk to the department – you make sure security is aware And your patient arrives.
More common in the setting of atherosclerotic lesions than emboli, which typically occur with sudden onset of symptoms. Symptoms may range from days to months prior to stroke onset. As many as two-thirds of patients with BAO experience prodromal symptoms, including TIAs, minor strokes, or other symptoms.
Smith comment: We have shown that use of opiates is associated with worse outcomes in ACS: Bracey, A. Smith comment: We have shown that use of opiates is associated with worse outcomes in ACS: Bracey, A. Opioids in ACS may reduce the pain score, but do not provide reperfusion for ongoing ACS. Abstract 556.
After developing encephalopathy and hypoxemic respiratory failure, the patient was transferred to the ICU. Further diagnostic testing in the ICU identified salicylate toxicity. Further diagnostic testing in the ICU identified salicylate toxicity. Available from: [link] Newman-Toker DE, Nassery N, Schaffer AC, et al.
It is also true that anterior and inferior T-wave inversion could be consistent with reperfusion of a type III wraparound LAD occlusion, despite the fact that Kosuge et al showed that T-wave inversion in lead III is much more likely to be PE than ACS if your differential contains nothing else. She was discharged and did well.
1 The American College of Surgeons’ (ACS) Trauma Quality Improvement Program (TQIP) Massive Transfusion in Trauma Guidelines leave a good amount of flexibility for hospitals regarding transfusion protocols, focusing more on systems-level aspects of designing and implementing MTPs.2,3 in the 1:1:1 group vs. 17.0% vs. 14.6%, p=0.03).
Intensivists have embraced the tracheostomy as an ICU procedure. doi: 10.21037/acs.2018.03.01. In a breaking from what could only loosely be described as tradition at this point, this podcast is going to be in 2 parts. It’s one of the most invasive and one of the riskier procedures we do. Surgical anatomy of the trachea.
She did not receive any opioids (which would mask her pain without affecting any underlying ACS). If for some reason the angiogram is delayed, they should receive maximal medical therapy in an ICU setting with continuous 12-lead ST segment monitoring under the close attention of a practitioner with advanced ECG interpretation training.
An example using a real case I had while on call in the ICU: A 61-year-old female had a post-induction arrest on the wards/hospital telemetry floor after being intubated for airway protection. Assigning a patient a single PCAC score upfront may implicitly bias clinicians familiar with the score in how they care for patients.
2 Amiodarone is commonly known for its anti-arrhythmic properties and a commonly used agent in the Intensive Care Unit (ICU). Sepsis, hyperthyroidism, dehydration, heart failure, ACS, etc). However, digoxin is known for its rate-control properties and its direct vagal effect on the atrioventricular node. Paper: Mason JM, et al.
Notable Physical Exam: General: Tripoding, severe respiratory distress. However, emergency physicians have recently faced a multitude of patients requiring ETI with anatomically and physiologically difficult airways; these patients increase the risk of a can’t intubate/can’t oxygenate scenario or significant hypoxemia, hypercarbia, or acidemia.
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chest pain. The cardiologists felt that the ECG did not represent ACS, and thought it was more likely pericarditis, so they did not take him to the cath lab. in the ICU but survived with excellent function.
The definition of massive hemoptysis is variable across publications with expectorated blood volumes ranging from 100 to 1,000 mL per 24 hours, as these volumes are difficult to estimate for any given patient. 2 Death from hemoptysis is akin to drowning, so airway considerations usually take precedence over hemodynamic considerations.
Below follows a drug manual for use in the CCU (coronary care unit), ICU (intensive care unit) or ER (emergency room). Gordon AC, Mason AJ, Thirunavukkarasu N, et al. Several endogenous and synthetic agents exist and are frequently combined to achieve the desired hemodynamic outcome. Minimal chronotropic effect. JAMA 2018; 319:1889.
I took part in her ICU care and she was extubated and stable to transfer to a stepdown unit after a few days. Patients like her are the reason we are advocating for a change in the ACS paradigm from STEMI to OMI. However, the prehospital ECG is more worrisome: the T-wave inversion in V5 and V6 is preceded by ST Elevation.
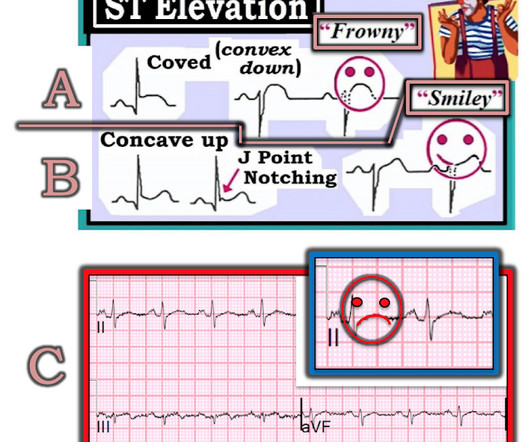
The patient was managed in the ICU and had serial troponins. An angiogram confirmed ACS as the etiology. You do NOT see this in normal variant STE, nor in pericarditis. The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." First was 2.9
The biggest change has been the gradual replacement of diacetylmorphine (heroin) by fentanyl and other synthetic opioids. Along the same time, a veterinary sedative, xylazine , became popular in Puerto Rico in individuals who used injection drugs [3]. We treat with wound care and reserve surgical management only for limbs that are no longer viable.
10 Although this is not the same pathophysiology seen in ACS from an acute plaque rupture leading to coronary artery occlusion, patients can have relatively abrupt coronary ischemia causing ACS due to acute, concentric vessel narrowing. BNP should normalize after about 2 months. 13 Cefepime 2 g or Piperacillin-Tazobactam 4.5
Goodman AD, Got CJ, Weiss AC. Introduction Crush injury: result of physical trauma from prolonged compression that initially causes direct tissue damage and later results in downstream effects from hypoxic conditions suffered by those tissues. 6 Motor vehicle collisions that produce significant challenges to passenger extrication.
In this situation, an ABG should be obtained periodically for correlation, though this is more relevant for the intensive care unit (ICU) setting than in routine ED care (5, 9). How would an ABG even change the initial stabilization of any of these patients? What alternative testing can be done in these circumstances?
Garabon JJW, Gunz AC, Ali A, Lim R. Every month we ask some of our friends from PERUKI (Paediatric Emergency Research in the UK and Ireland) to point out something that has caught their eye. This time the PEM MSc team from QML , in association with DFTB, are taking over… Article 1: Insulin infusion in paediatric DKA – high or low?
Left lower lung field end demonstrates expiratory wheezing on auscultation. Other lung fields unremarkable. smoke, high ozone levels, smog) Asthma/reactive airway disease (RAD) Diagnostic criteria 7,8 Respiratory symptoms +/- fever (at least 38.0 C or 100.4 mg/kg, max 4 mg per dose q20-30min) or hydromorphone (0.01-0.02 mg/kg, max 0.4 C or 100.4
Disposition is often admission to an intensive care unit (ICU) setting. Questions: What is the most likely causative xenobiotic that led to these findings? Influenza vaccine Methanol Organophosphate Paraquat Are her symptoms reversible? Yes No What therapy or therapies are critical for this patient? 7 May lead to respiratory failure.
This process of sickling and unsickling goes on and off until the erythrocyte membrane is no longer flexible. Irreversible sickle cells undergo either intravascular haemolysis or extravascular removal by the reticulo-endothelial system resulting in anaemia and splenic sequestration. Blood culture is pending. How would you evaluate this child’s pain?
Paper: Alwang AK, Law AC, Klings ES, Cohen RT, Bosch NA. To assess the clinical impact and relevance of these concerns, Alwang et al. performed the retrospective cohort study below ( Alwang 2024 ). Lactated Ringer vs Normal Saline Solution During Sickle Cell Vaso-Occlusive Episodes. JAMA Intern Med. 2024;184(11):1365-1372.
It’s easy to think of bacteria as always “wanting” to infect a host as quickly and aggressively as possible (and if you’ve ever taken care of someone with an acute PA bloodstream infection, you know how fast they can go from healthy to needing the ICU). Yes, that’s right. 2-AA helps PA do just that.
History of Present Illness The collateral history indicates that her symptoms began one week into her journey, but medical care was inaccessible at the time. The family reports no history of food allergies, insect bites, or contact with sick individuals. The patient did not receive pre-travel prophylaxis for malaria, hepatitis A, or yellow fever.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content