This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." The patient was upgraded to the ICU for closer monitoring. looked at consecutive patients with PE, ACS, or neither. Kosuge et al. Witting et al. of controls.
Moreover, the Queen is only supposed to be used with a high pretest probability of ACS/OMI. The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course. Is it STEMI? We just finished training version 2 with some cases of hypokalemia, so that is in the future.
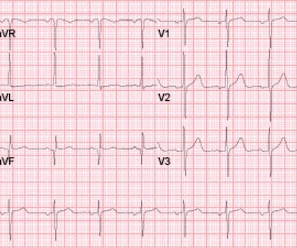
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
Authors state early cath may be of benefit in those with no STEMI, but much of the more recent literature suggests this is more controversial. Statements: In ICUs where advanced cerebral monitoring is not in routine use, target an MAP >80 mm Hg unless there are clinical concerns or evidence of adverse consequences (82.6%, 19/23).
Immediate and early percutaneous coronary intervention in very high-risk and high-risk Non-STEMI patients. Smith comment: We have shown that use of opiates is associated with worse outcomes in ACS: Bracey, A. Opioids in ACS may reduce the pain score, but do not provide reperfusion for ongoing ACS. Lupu L, et al.
An example using a real case I had while on call in the ICU: A 61-year-old female had a post-induction arrest on the wards/hospital telemetry floor after being intubated for airway protection. PMID: 30060961 Koller AC, et al. In a PCAC 1 or 2, we may prioritize a cath and tolerate a couple hours without ICU Neuroresuscitation.
I took part in her ICU care and she was extubated and stable to transfer to a stepdown unit after a few days. Patients like her are the reason we are advocating for a change in the ACS paradigm from STEMI to OMI. Her repeat ECHO showed an improving EF of 37%.
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chest pain. The cardiologists felt that the ECG did not represent ACS, and thought it was more likely pericarditis, so they did not take him to the cath lab. in the ICU but survived with excellent function.
The patient was managed in the ICU and had serial troponins. An angiogram confirmed ACS as the etiology. (THE PM CARDIO OMI AI APP) If you want this bot to help you make the early diagnosis of OMI and save your patient and his/her myocardium, you can sign up to get an early beta version of the bot here. He had no more ECGs recorded.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














Let's personalize your content