This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Clinical impact: Rather than arguing with the patient about the likelihood of this phenomenon occurring and whether this is a true allergy, the patient is informed that they do not need to immediately start treatment to receive care in the hospital. DOI: Papudesi BN, Malayala SV, Regina AC. 2023 Aug 1;89(2):231. Xylazine toxicity.
A thorough review of vital signs, physical exam findings and a complete blood count with differential, renal function panel and urinalysis offer valuable information in the patient being worked up for HUS. This of course, is made easier if you can get a stool sample to analyze in the first place.
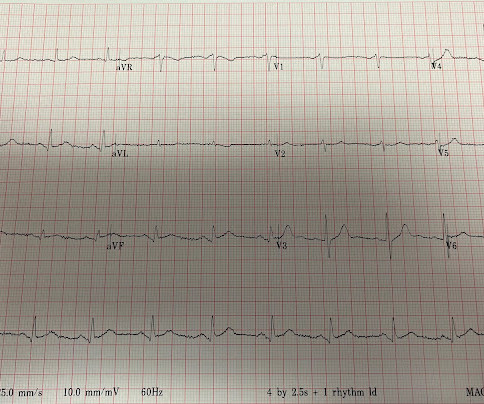
ACS would be highly unusual in a young athlete, and given the information on his race bib, one must first suspect that the abnormal ST elevation is due to demand ischemia, not ACS. A bedside echo performed by the emergency physician showed no wall motion abnormality and confirmed LVH.
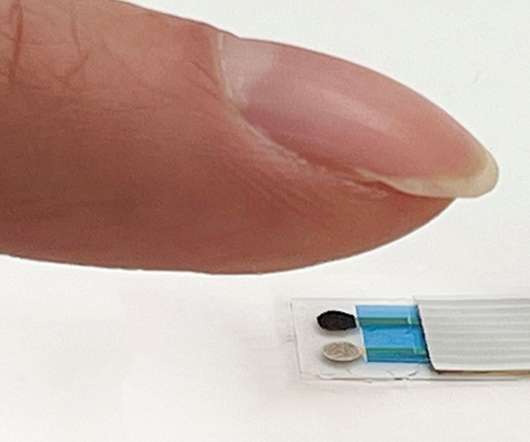
“Through a single touch, our new device can obtain clinically useful molecular-level information about what is circulating in the body,” said Sam Emaminejad, another researcher involved in the study. ” The researchers presented their technology at the 2022 fall meeting of the American Chemical Society (ACS). .
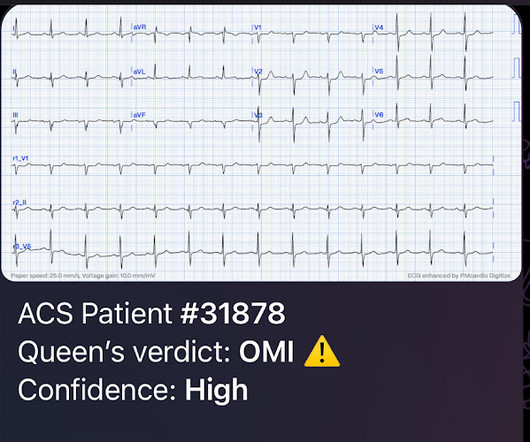
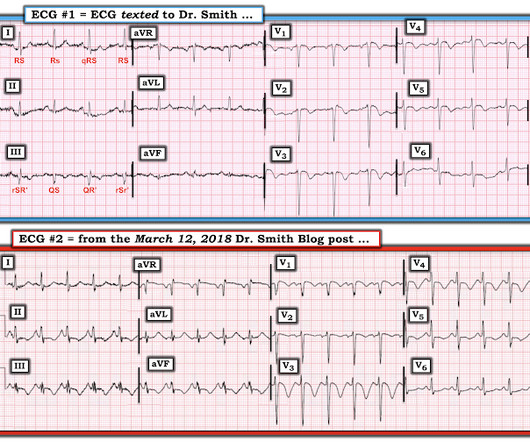
This was texted to me from a former resident, while working at a small rural hospital, with the statement: "I can’t convince myself of anything here, but he’s a 63-year-old guy with prior stents and a good story for ACS." I sent it to Pendell, and he said OMI with low confidence without any other information.
Sent by anonymous, written by Pendell Meyers I received a text with this image and no other information: What do you think? The person I was texting knows implicitly based on our experience together that I mean "Definite posterior OMI, assuming the patient's clinical presentation is consistent with ACS."
If this EKG were handed to you to screen from triage without any clinical information, what would you think? showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS. looked at consecutive patients with PE, ACS, or neither.
What would you do at this time with this information? But pain is an important signal in MI and informs the clinician of the urgency. Smith : As Willy states, ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). At midnight. A few notes: Morphine treats ALL forms of pain.
This is a particularly informative link: 2 Examples of Posterior Reperfusion T-waves So one might think that, with active pain, there is anterior OMI. Comment : ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). I think the ECG is normal.
If there were diffuse ischemic STD, with precordial STDmaxV5-6 and reciprocal STE-aVR, this would be non-specific subendocardial ischemia from ACS or supply-demand mismatch. The new ESC guidelines has for the first time merged both STEMI and non-STEMI in the same guideline because they are both on the spectrum of ACS.
119.042891 Ashburn NP, Snavely AC, O’Neill JC, et al. 2018.05.040 Featured image adapted from Adobe Firefly Author information Matthew J.W. 2021 Jun 22;143(25):e1118]. Circulation. 2019;140(19):1543-1556. doi: 10.1161/CIRCULATIONAHA.119.042891 J Am Coll Cardiol. 2018;72(6):620-632. doi: 10.1016/j.jacc.2018.05.040
An expert committee appraised the evidence behind recommendations to avoid imaging to inform the 2022 NICE guidance. Discussion may be supported by patient information materials, particularly the provision of information in multiple languages. doi:10.1177/0883073818786086 Young AC, Costanzi JB, Mohr PD, Forbes WS.
This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. I sent it to 5 of my OMI friends without any clinical information or outcome and all 5 independently responded with exactly the same diagnosis: "reperfused inferior OMI". There is ischemic ST depression in V4-V6.
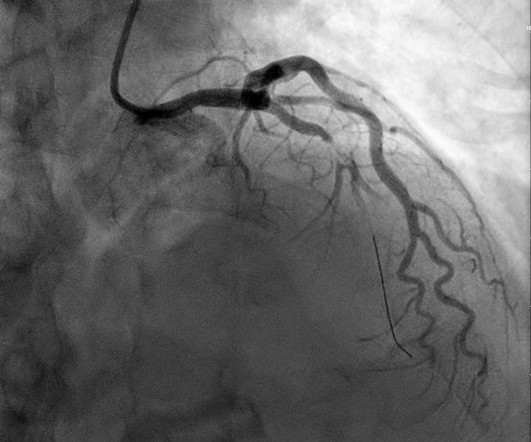
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Optical coherence tomography, due to its high resolution, may provide additional information [ 10,13 ]. References: 1.
Article: Vaeli Zadeh A, Wong A, Crawford AC, Collado E, Larned JM. It’s not mentioned whether the authors attempted to identify additional studies by checking the references of the selected articles or by contacting the original paper authors for more information.
ACS surgeons appeared to select surgery as their initial choice substantially more frequently than other subspecialties. ACS surgeons would have sent 6/43 patients for ERCP or MRCP (14%), whereas surgical oncologists would have sent a higher percentage of patients for ERCP or MRCP (7/18 or 38.9%).
I texted this ECG with no information to Dr. Smith, who immediately said: "If CP, then anterior OMI until proven otherwise." References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Am Heart J.
He sent it to me with no other information and I wrote back "100% diagnostic of LBBB with inferior-posterior-lateral OMI" There is atrial paced rhythm with Left Bundle Branch Block (LBBB). The cath report showed: Significant stenosis with subtotal occlusion (99%) in the prox to mid Lcx, culprit of ACS, TIMI flow 1.
Written by Pendell Meyers Both of these cases were sent to me with no information other than adults with acute chest pain. What would be your response? Case 1: Case 2: What if I told you that Case 1 has an abnormal initial troponin, and Case 2 has a normal initial troponin? Case 1 An elderly male presented with chest pain.
Learning points: Both patients and other medical providers can report confusing and often contradictory information that obfuscates the diagnosis (in this case, WPW). Although recognition of OMI was not affected by administration of morphine in this case, use caution with analgesia in ongoing ACS without a definitive plan for angiography.
This is supplied via alternating current (AC), increasing the risk of titanic contraction of skeletal muscle, leading to kids holding on to the electrical power source. AC and DC shocks may result in different injury patterns. Significant injuries can occur even in the absence of extensive burns or other signs of external injury.
The measure, developed in collaboration with the American College of Surgeons (ACS), the Institute for Healthcare Improvement (IHI) and the American College of Emergency Physicians (ACEP), aims to improve older adult patient care and outcomes. Read this CMS fact sheet for more information about the rule (see p.
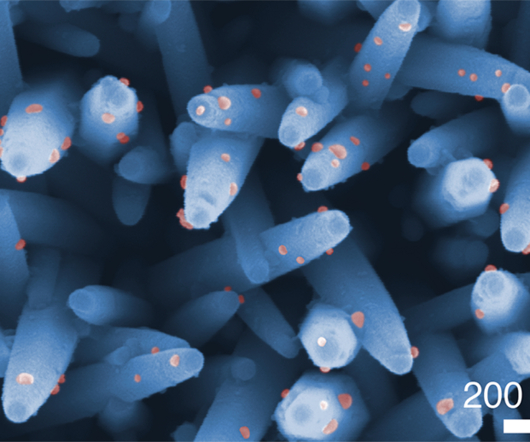
Urine tests are an effective, simple, and non-invasive method because the urine contains many informative biomolecules that can be traced back to identify the disease.” Study in ACS Nano : All-in-one nanowire assay system for capture and analysis of extracellular vesicles from an ex vivo brain tumor model Via: Nagoya University
An ECG was texted to me (Smith) without any clinical information: What did I say? This clinical information followed: "The patient had a COPD exacerbation with a prehospital SpO2 of 60%. This clinical information followed: "The patient had a COPD exacerbation with a prehospital SpO2 of 60%. This is NOT Wellens. Kosuge et al.
Hopefully in a few minutes you’ll at least have a few morsels more of information to stave off all the trainees who are undoubtedly much smarter than you on the ward round. Type 1 is the acute deterioration in kidney function seen in cardiogenic shock from ACS. Today we tackle a somewhat nebulous syndrome.
2020.09.082 Full prescribing information. link] Full prescribing information. link] Li Z, Krippendorff BF, Sharma S, Walz AC, Lavé T, Shah DK. Unified Treatment Algorithm for the management of crotalid snakebite in the United States: results of an evidence-informed consensus workshop. Ann Emerg Med. 2020;76(4):S29.
There were zero patients in this study with a "normal" ECG who had any kind of ACS! This defies all previous data on acute MI which would show that even undetectable troponins do not have a 100% negative predictive value. So this study is actually worthless.
The patient has ACS by history, active pain, and an elevated troponin. Fortunately, ECG is not the only diagnostic information to clue you into the possibility OMI! It is impossible to overstate the importance of putting the ECG and troponin into the context of the clinical history. Smith : at this point, the ECG becomes irrelevant.
Smith: If this is ACS (a big if), t his is just the time when one should NOT use "upstream" dual anti-platelet therapy ("upstream" means in the ED before angiography). History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Anything more on history?
With no other information other than the first ECG above, I texted this to Dr. Smith and he responded: ST elevation in lead V2 and terminal QRS distortion in V3. See this study showing an association between morphine and mortality in ACS: Use of Morphine in ACS is independently associated with mortality, at odds ratio of 1.4
After rethinking the case, he remained concerned about ACS and subsequently performed a point-of-care ultrasound in order to evaluate for regional wall motion abnormality. We do not know whether a better assay would have given better information, but it is very likely. There is no age cut-off for ACS. Do NOT use them.
Assessing the Severity The severity of an electrical burn depends on several factors: the type of current (AC or DC), voltage, the pathway of the current through the body, the duration of contact, and the victim’s overall health. It helps in making informed decisions for the next steps in treatment.
MOREVER, the morphology of the TWI is just not right for ACS. showed that, when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS. S1Q3T3 This is a paper worth reading : Marchik et al. They found that S1Q3T3 had a Positive Likelihood Ratio of 3.7,
If this is ACS with Aslanger's pattern , the ST depression vector of subendocardial ischemia (due to simultaneous 3 vessel or left main ACS) is directed toward lead II (inferior and lateral). Also, ACS does not cause hypoxemia out of proportion to hemodynamic compromise, as PE can.
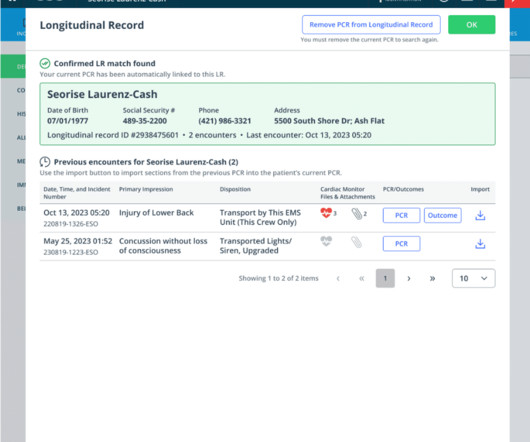
Now, any agency unit (not aiding agency units) can be re-dispatched from the Units Report page with separate information (times, personnel, actions) completed for each re-dispatched unit report. Injury Prevention Summary ACS PRQ- Hospice ACS PRQ – Solid organ injuries PtReg: 2.5 Neurosurgeon Response PRQ- 2.12
I did not have more information at the time. I remained unconvinced that this was due to ACS. With the added history, and the entirety of the presentation, it was determined by cardiology that the clinical presentation was not due to ACS. Is there a formula to help with this? See discussion at the bottom.
Remember that the ECG reports what is happening to the myocytes , then you must use that information to make inferences about what the patient needs. One must always be careful when looking for "baseline" ECGs, because the prior ECG on file may have been during another ACS event, as this one clearly was.
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. This case represents the same physiologic event as OMI in terms of the result on the myocardium, therefore with identical ECG features, however there may not be ACS!
Corroborating this is the subtle ST depression in V2-V3 which is inappropriate for the normal QRS complex, and in the context of ACS, we have shown this is quite specific for posterior OMI. I sent the ECG with no information to Dr. McLaren, who instantly replied: "RCA?" (he he means, "inferoposterior OMI, so probably RCA occlusion?").
Thus, the very well informed physician could differentiate these ECGs from those of an LBBB patient with MI: 1) no concordance 2) no excessive discordance 3) LBBB with tachycardia, probably rate related 4) subsequent T wave inversion that, according to Shvilkin et al., link] Shvilkin et al. mm, and T-wave inversion in lead III is only 2.5
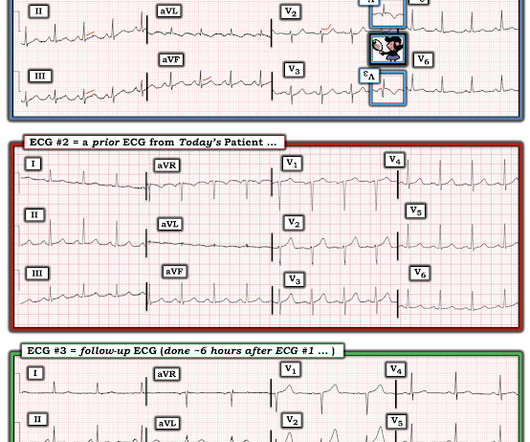
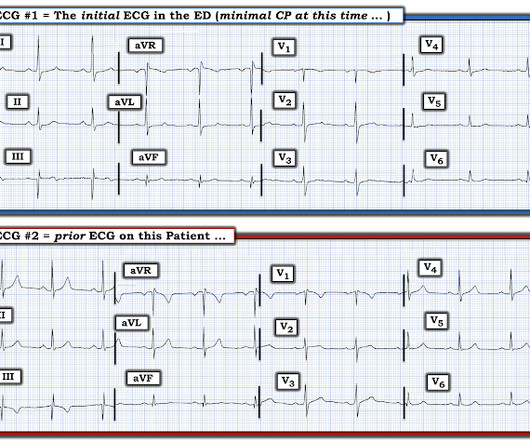
Meyers : I was sent this ECG with zero clinical information (and without the prior ECG below), and at that time I said that I did not see evidence of OMI. Only if you are uncertain about the diagnosis of ACS. Initial vitals: Temp 36.7 C, BP 161/79, RR 16, HR 70, Pulse Ox 97% Initial ECG (during "minimal" pain): What do you think?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content