This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The post JJ 16 Heparin for ACS and STEMI appeared first on Emergency Medicine Cases. Does heparin - LMWH or unfractionated heparin - benefit the patient with a pretty good story for angina with a bump in their troponin and some ST depression in the lateral leads? And for STEMI too. But should we? But should we?
Thus, the lumen observed may actually still be the same size as the original, normal lumen. Furthermore, in studies reporting progression of insignificant lesions to total thrombotic occlusions, the mean interval between angiography and acute myocardial infarction is 2.5 years, with the interval as long as 12 or 18 years in some studies.
Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates). Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates). The CXR demonstrated no pulmonary edema.
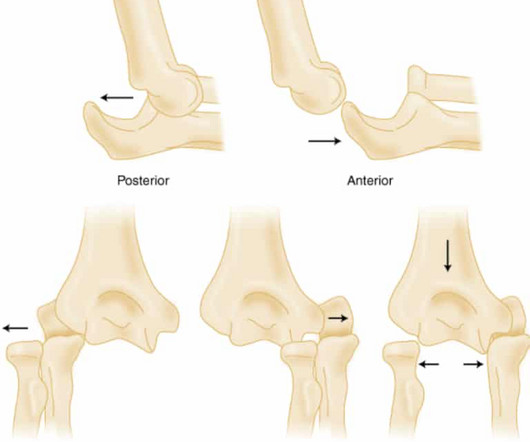
Elbow Dislocation Definition: Disarticulation of the proximal radius & ulna bones from the humerus Epidemiology: Incidence Second most common joint dislocation (after shoulder) in adults Most commonly dislocated joint in children Accounts for 10-25% of all injuries to the elbow ( Cohen 1998 ) Posterolateral is the most common type of dislocation (..)
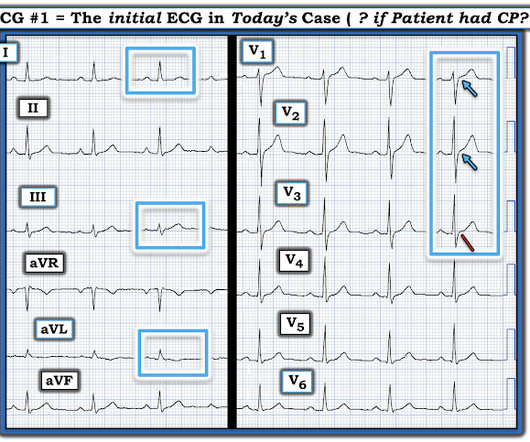
As a result, even before looking at this patient's initial ECG — he falls into a high -prevalence likelihood group for ACS ( for an A cute C oronary S yndrome ). We therefore need to assume and rule "out" ACS — more than having to rule it "in". The "onus of proof" remains on us as medical providers to objectively rule out ACS.
The biggest change has been the gradual replacement of diacetylmorphine (heroin) by fentanyl and other synthetic opioids. Along the same time, a veterinary sedative, xylazine , became popular in Puerto Rico in individuals who used injection drugs [3]. We treat with wound care and reserve surgical management only for limbs that are no longer viable.
Pediatric Buckle and Greenstick Forearm Fractures: Basics The junction of the metaphysis and diaphysis in pediatric long bones is an area of biomechanical transition (Light, 1984) Thin metaphyseal cortex meets the thick cortex of the diaphysis Or in Emergency Medicine terms, “ Thick bone meet thin bone.” J Bone Joint Surg Br. 2001;83:1173-5.
What are the most useful historical factors to increase and decrease your pretest probability for ACS? Which cardiac risk factors have predictive value for ACS? Why should the words "troponitis" and "troponemia" be banned? How should high sensitivity troponin be interpreted differently than conventional troponin? and many more.
You turn to the attending and ask, “do you really think this could be acute coronary syndrome (ACS)?” ACS is usually amongst this differential, as cardiovascular disease is a leading cause of morbidity and mortality in this population. The proportion of patients with ACS at the index visit or within 30 days. *
ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock. Then ACS (STEMI) might be primary; this might be cardiogenic shock. One must clearly rule out these processes before jumping on the ACS diagnosis. Are the lungs clear? Is the patient cool and pale? Large volume fluid resuscitation was undertaken.
Then assume there is ACS. Therefore — recognition of DSI on ECG should prompt consideration of 2 Categories of diagnostic entities : Severe Coronary Disease ( due to LMain, proximal LAD, and/or severe 2- or 3-vessel disease ) — which in the right clinical context may indicate ACS ( A cute C oronary S yndrome ).
Welcome to the first episode of the Broomedocs podcast for 2025. Justin and I are back for more nerdy goodness to make you smarter in the Resus room, or at a pub trivia night more likley… wether it is about salt correction, dissection or infection we can help you out! Listen in and learn! Dimer is useful in the low risk group. Emerg Med J.
Although the attending crews did not consider the ECG pathognomonic for occlusive thrombosis, they nonetheless considered the patient high-risk for ACS and implored him to reconsider. The attending crews were concerned for an ACS-equivalent of LAD occlusion and initiated a prehospital STEMI activation to the closest PCI center.
Jonklaas J, Bianco AC, Bauer AJ, Burman KD, Cappola AR, Celi FS, Cooper DS, Kim BW, Peeters RP, Rosenthal MS, Sawka AM; American Thyroid Association Task Force on Thyroid Hormone Replacement. The patient had no significant past medical history. She also endorsed three weeks of cough and congestion, and one day of muffled voice. Pediatr Rev.
Takeaway lessons * If considering ACS in any post-menopausal woman, you should also consider stress cardiomyopathy. Of course, atypical anatomical distributions can also occur in ACS due to distinct anatomy. ACE inhibition). * In general, TCM is a diagnosis of exclusion after ruling out ACS. Find us on Patreon here!
This was texted to me from a former resident, while working at a small rural hospital, with the statement: "I can’t convince myself of anything here, but he’s a 63-year-old guy with prior stents and a good story for ACS." Chest pain or discomfort) What do you think? Here was my response: "Suspicious for inferior posterior OMI.
ACS would be highly unusual in a young athlete, and given the information on his race bib, one must first suspect that the abnormal ST elevation is due to demand ischemia, not ACS. His initial ECG is shown here. A bedside echo performed by the emergency physician showed no wall motion abnormality and confirmed LVH.
A healthy 45-year-old female presented with chest pain, with normal vitals. The computer interpretation was “ST elevation, consider early repolarization, pericarditis or injury.” What do you think? There’s normal sinus rhythm, normal conduction, borderline right axis, and normal voltages. There’s TWI in aVL but this is concordant to its QRS.
These have all been small studies, studying very few patients with ACS, and often used final cardiology interpretation rather than patient outcome. Smith : This study had such low risk patients that not a single patient was ultimately diagnosed with ACS. It is well known that NOMI usually has a normal ECG or nonspecific ECG.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). ACE inhibitors, or potassium-sparing diuretics), are particularly susceptible. In the case of ACS, the ECG can rapidly change from this. Past medical history included HTN, HLD, and MI 10 years prior.
If there were diffuse ischemic STD, with precordial STDmaxV5-6 and reciprocal STE-aVR, this would be non-specific subendocardial ischemia from ACS or supply-demand mismatch. The new ESC guidelines has for the first time merged both STEMI and non-STEMI in the same guideline because they are both on the spectrum of ACS.
Comment : ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). The ESC states that patients with suspected ACS should go to the cath lab in <2 hours "regardless of ECG or biomarker evidence of MI!!" There are no hyperacute T waves. There is no inappropriate ST depression.
The bottom line from that episode was that the HEART Pathway appears to have the potential to safely decrease objective cardiac testing, increase early discharge rates and cut median length of stay in low-risk chest pain patients presenting to the ED with suspicion of ACS. If we thought about ACS, we brought them in. AEM June 2022.
This should prompt immediate investigation into supply-demand mismatching, or ACS. There is bradycardic Atrial Fibrillation with broad ST-depression in most leads and perceptible ST-elevation in aVR. But there’s some peculiar features about this ECG: The unusually short QT The “scooped out” appearance of the ST-segments.
Exclusion criteria: Transferred patients, HR <40 or >140 bpm, SBP <90 or >180 mmHg, RR <6 or >36/min, GCS <15, possible ACS, headache, pregnancy, breastfeeding, known renal or hepatic failure, previous malignant hyperthermia, known sensitivity to fluorinated anesthetics, or agitated/aggressive per nursing staff.
Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients. She arrives in the emergency department (ED) with decreased level of consciousness and shock. The EKG shows sinus tachycardia with nonspecific changes and no ST segment elevations, Q waves, or hyperacute T waves.
Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? If you are worried about aortic dissection, you also want the BP to be lowered, though you would do it first with esmolol to decrease the dP/dT (change in pressure over change in time). The ST depressions in I and aVL have resolved. Smith: What???!!!
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. Smith : This is ACS even if the troponin returns normal, and the first troponin especially might return normal. This results in Type I MI. This results in Type II MI. Severe HTN d.
The patient was thought to have low likelihood of ACS, and cardiology recommended repeat troponin, urine drug testing, and echocardiogram. At that point, cardiology elected to treat for ACS. Initial hscTnI was 10 ng/L (ref. <14). There was no recommendation for repeat ECG. Angiography is shown below.
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. It is not yet available, but this is your way to get on the list. link] Case continued She arrived in the ED and here is the first ED ECG.
As per my review of this subject ( Check out My Comment at the bottom of the page in the November 16, 2023 post in Dr. Smith's ECG Blog ) — the 3 most common Causes of ACS ( A cute C oronary S yndrome ) with a "negative" cath are: i ) Myocarditis; ii ) Takotsubo cardiomyopathy; and , iii ) MINOCA.
The Eastern Association for the Surgery of Trauma (EAST) , the National Association of EMS Physicians (NAEMSP) , and the American College of Surgeons Committee on Trauma (ACS-COT) all support the recommendation against the use of spinal immobilization in patients with isolated penetrating injuries. to prevent movement of the spine.
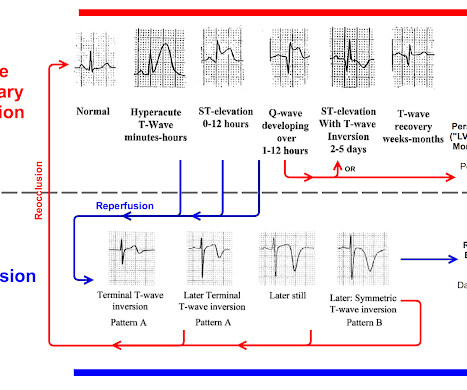
You must understand this and the dynamic nature of ACS to provide excellent care for such patients. Here is the OMI progression of ECG findings for review: You can see that OMI ECG findings must "deflate" and pass through normal or near-normal in order to get to reperfusion findings. This is termed " pseudo-normalization."
VS abnormalities can drive this as well Strongly consider reversal of AC (this will typically come after control) Stopping the Bleeding PPE: these things bleed like stink. Take Home Points: Posterior epistaxis is a rare, life-threatning presentation. Literature doesn’t defend this approach but, the lit is pretty sparse.
Episode written by Jeff Kott and Tony Breu Kott J, Cooper AZ, Breu AC, Abrams HR. Nephmadness 2024. The Curious Clinicians Podcast. March 4th, 2024. Image source: [link]
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Link to abstract Link to full text 2) Use of Morphine in Non-STE-ACS is independently associated with mortality, at odds ratio of 1.4
He had no symptoms of ACS. His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS." A troponin this high in a patient with no known chronic troponin elevation, and active acute ACS symptoms, has a very high likelihood of type 1 ACS regardless of the ECG.
Study in journal ACS Sensors : Rapid Direct Detection of SARS-CoV-2 Aerosols in Exhaled Breath at the Point of Care Via: Washington University School of Medicine The technology requires someone to breathe into it just once or twice, and it can then provide an indication if the person is infected with SARS-CoV-2 in as little as one minute.
The faculty physician thought this is highly likely to be ACS. Here is his ECG: He had a previous ECG on file, from many years prior: What do you think? There is new T-wave inversion in inferior leads and V3-V6. This is recorded during pain. However, most T-wave inversion during pain is nonspecific.
Acute chest syndrome (ACS) is a potentially life-threatening complication of sickle cell disease characterized by lung infiltrates, fever, and respiratory symptoms, including cough, tachypnea, wheeze, increased work of breathing or shortness of breath, and reduced oxygen saturation. Sickle cell disease is the primary risk factor for ACS.
He had been smoking an opiate and suddenly collapsed. He was ventilated with BVM on arrival. He awoke with naloxone. This EKG was recorded as part of a standing order for critical care. He denied any CP or SOB. An EKG was repeated at 5 minutes The T-wave is less hyperacute. Maybe there is some spontaneous reperfusion? It does not radiate.
Each article will take a deeper dive into each recommendation’s supporting evidence and practical implications. Do not order laboratory testing or a CT scan of the head for a patient with an unprovoked, generalized seizure or a simple febrile seizure who has returned to baseline mental status. What is the evidence for avoiding imaging?
But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Potassium was normal.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content