This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
And for STEMI too. The post JJ 16 Heparin for ACS and STEMI appeared first on Emergency Medicine Cases. Does heparin - LMWH or unfractionated heparin - benefit the patient with a pretty good story for angina with a bump in their troponin and some ST depression in the lateral leads? But should we? But should we?
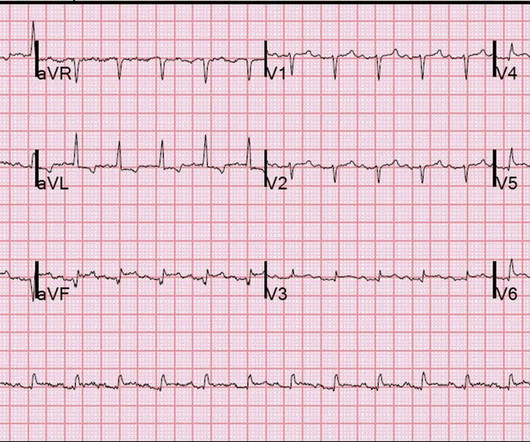
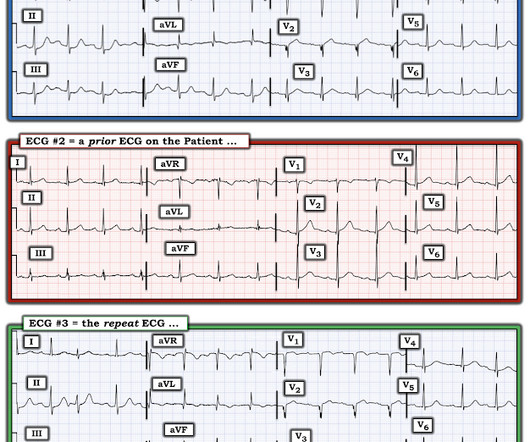
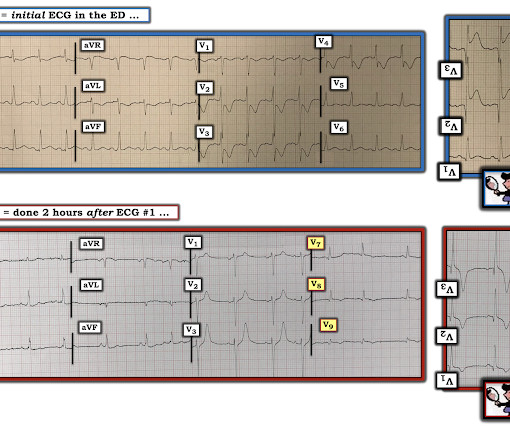
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. He does have a recently diagnosed PE, and has not been taking his anticoagulation due to cost. He had a previous ECG on file: Proving the findings are new The cath lab was activated. He was given aspirin and sublingual nitro and the pain resolved.
Because the most severe LAD OMIs can cause ischemic failure of the RBB and LAF, any patient with ACS symptoms and new RBBB and LAFB with any concordant STE has LAD OMI until proven otherwise. There is no recognition of STEMI equivalency in this setting in the USA guidelines currently. Long term outcome is unavailable.
He was rushed by residents into our critical care room with a diagnosis of STEMI, and they handed me this ECG: There is sinus tachycardia with ST elevation in II, III, and aVF, as well as V4-V6. At first glance, it seems the patient is having a STEMI. ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock.
These have all been small studies, studying very few patients with ACS, and often used final cardiology interpretation rather than patient outcome. Smith : This study had such low risk patients that not a single patient was ultimately diagnosed with ACS. It is well known that NOMI usually has a normal ECG or nonspecific ECG.
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. Do NOT give it unless you are committed to the cath lab!! Cath attending is aware. It is a mass delusion.
Based on recent studies, current guidelines recommend that O2 should not be given to non-hypoxemic patients with STEMI or NSTEMI [2,3]. REBEL Cast Ep114 – High Flow O2, Suspected ACS, and Mortality? 4159 patients (10% of total population) had STEMI 30d Mortality: High O2 protocol: 8.8% Low O2 protocol: 3.1%
Then assume there is ACS. Cardiac arrest #3: ST depression, Is it STEMI? The ST depression usually resolves, or is clearly resolving (getting much better). Just as important is pretest probability: did the patient report chest pain prior to collapse? This may or may not be true, but it should give you pause.
Although the attending crews did not consider the ECG pathognomonic for occlusive thrombosis, they nonetheless considered the patient high-risk for ACS and implored him to reconsider. A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. A 12 Lead ECG was recorded.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Smith : As Willy states, ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC).
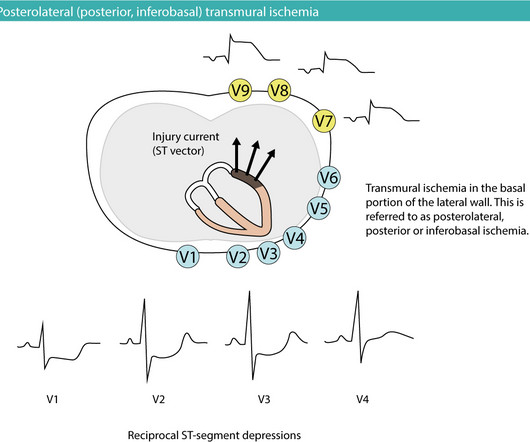
Posterior (posterolateral) acute myocardial infarction (STEMI) The heart is rotated 30° to the left in the thorax. One might wonder what the probability is that the patient actually has NSTE-ACS (NSTEMI) since they present with ST segment depressions on the 12-lead ECG (recall that ST segment depression is the hallmark of NSTE-ACS/NSTEMI).
The cardiologist recognized that there were EKG changes, but did not take the patient for emergent catheterization because the EKG was “not meeting criteria for STEMI”. Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? The ST depressions in I and aVL have resolved. Smith: What???!!!
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
There were zero patients in this study with a "normal" ECG who had any kind of ACS! So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. Deutch et al.
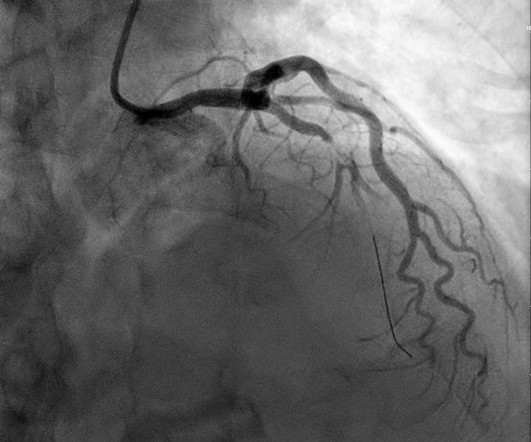
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. It is not yet available, but this is your way to get on the list. link] Case continued She arrived in the ED and here is the first ED ECG.
Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients. There is evidence that taking those patients with ROSC and EKG showing STEMI directly for angiography +/- angioplasty is associated with positive patient-oriented outcomes.
Discharge ECG showed antero-inferior reperfusion T wave inversion: Had the initial ECG been signed off as “STEMI negative” the patient could have arrested in the waiting room, with a poor cardiac and neurological outcome. A healthy 45-year-old female presented with chest pain, with normal vitals. What do you think? But which one is it?
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). There is mixed overlap of ST-segment elevation (STE), ST-segment depression (STD), Hyperacute T waves (HATW), and deWinter pattern (which the ACC regards as a STEMI-equivalent but is better suited under the blanket of OMI).
Many conditions outside of acute coronary syndrome (ACS) mimic ST-elevation myocardial infarction (STEMI), but only a handful of cases have reported ST-elevations (STE) in the setting of pancreatic inflammation where underlying ACS was excluded. The Case FIGURE 1: Initial EKG were notable for a leukocytosis of 23.19
I sent this ECG to the Queen of Hearts (PMcardio OMI), and here is the verdict: You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form Then I learned that a Code STEMI was activated for concern of anterior "STEMI" in V1-V2. High sensitivity troponin I was 23 ng/L.
ACS would be highly unusual in a young athlete, and given the information on his race bib, one must first suspect that the abnormal ST elevation is due to demand ischemia, not ACS. Thus, this patient had increased ST elevation (current of injury) superimposed on the ST elevation of LVH and simulating STEMI.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. This case is an example of the steps we can all take in daily practice as the paradigm shifts from STEMI to OMI.
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS. In fact, Kosuge et al. Stein et al.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. Potassium was normal. This is not unusual. Take home 1.
Comment : ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). The ESC states that patients with suspected ACS should go to the cath lab in <2 hours "regardless of ECG or biomarker evidence of MI!!" There are no hyperacute T waves. There is no inappropriate ST depression.
BP 142/100 HR 90 RR 16 (BBS CTA) SpO2 99 (RA) Dstick 110 My colleagues noted the ST-depression in the respective leads, as well, and STEMI activated to the nearest PCI center. 1] Here is the admitting ED ECG after cancellation of Code STEMI. Furthermore, there was no family history of early CAD, MI, or sudden cardiac death. is present.
Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Day 12 ECG: FINAL DIAGNOSIS: "NSTEMI" Despite the fact that his day 4 ECG easily meets STEMI criteria, the patient is diagnosed as NSTEMI. Am Heart J. 2005;149:1043–1049. link] Bracey, A.
This is a 45 yo male who had an inferior STEMI 6 months prior, was found to have severe LAD and left main disease, and was supposed to be set up for CABG a few weeks later, but did not follow up. But it could be anterior STEMI. 40% of anterior STEMI has upward concavity in all of leads V2-V6. is likely anterior STEMI).
This ECG was read as “No STEMI” with no prior available for comparison. It is true this ECG does not meet STEMI criteria (there is 1.0 The Queen of Hearts sees it of course: Still none of these three ECGs meet STEMI criteria. Do you think we discussed this patient's 2-3 hour delay to reperfusion in our quarterly "STEMI meeting"?
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). With EMS, patient had a GCS of 3 and was saturating 60% on room air. or basilar ischemia.
He had an immediate ED ECG: There is artifact, but the findings appear to be largely gone now The diagnosis is acute MI, but not STEMI. See this post on the (Five primary patterns of ischemic ST depression, without ST elevation) Because of the dynamic ACS, we activated the cath lab in the middle of the night. was much higher.
You can see how V1, V2, aVR, and V4R would have ST elevation in either a right ventricular STEMI or with a septal STEMI, and how lateral leads, and even posterior leads, would have reciprocal ST depression. of patients with anterior STEMI, ST elevation of greater than or equal to 3.0 STE in V4R is confirmatory evidence.
He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. Sensitivity was 87% for OMI in our validation study (it was 34% for STEMI criteria). So it can miss some OMI.
All patients with NSTE-ACS ( NSTEMI or unstable angina) are treated similarly with respect to anti-ischemic and anti-thrombotic drugs. Guidelines recommend the use of validated risk models to estimate the risk of acute myocardial infarction , 30-days and 1-year mortality in patients with NSTE-ACS.
This is as clear a STEMI as you can get. Now, it is true that shortly after a non-ACS cardiac arrest, there can be transient diffuse ST depression, but not ST elevation in a coronary distribution, and there should not be a wall motion abnormality. So this is classic inferoposterior STEMI on the ECG but is NOT acute coronary syndrome!
This patient could have very easily been overlooked, both because the ECG was STEMI negative and because the Q waves were attributed to an “old infarct”. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion. OMI or STEMI? As cardiology documented, “possible STEMI.
Furthermore, the term "STEMI equivalent" has no reliable or definable meaning except between two practitioners who both agree on the list of entities that they believe are STEMI equivalents and can agree on how to identify it. Here is his triage ECG when he presented at 1657: What do you think? J ACC 61(4):e78-140; page e83.
The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Similarly, the OMI paradigm respects ACS as a dynamic process in which ECG changes reflect the phase of myocardial injury and risk stratify which patients may benefit from emergent PCI. Is there STEMI? Leave it alone.
He had multiple cardiovascular risk factors and the EM physician strongly suspected ACS. Over the next few hours, four other general cardiologists "signed off on the initial ECG without recognizing STEMI." Learning Points: STEMI criteria misses 25-40% of OMI, like this case for example. mm of the "required" 1.0
He had no symptoms of ACS. The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS." Physician: "No STEMI."
The Queen of Hearts agrees: Here the Queen explains why: However, it was not interpreted correctly by the providers: ED interpretation of ECG: "paced rhythm, LBBB but no STEMI pattern." Most large STEMI have peak troponin I in the 20.0 HPI: Abrupt onset of substernal chest pain associated with nausea/vomiting 30 min PTA. ng/mL - 80.0
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? This is the response he got: Interventionist: "No STEMI, no cath. After stabilizing the patient and recording more ECGs, he tried again: Interventionalist: "It isn't a STEMI." It is a STEMI equivalent. We don't know how many though.
There’s mild inferior ST elevation in III that doesn’t meet STEMI criteria, but it’s associated with ST depression in aVL and V2 that makes it diagnostic of infero-posterior Occlusion MI (from either RCA or circumflex)– accompanied by inferior Q waves of unknown age. Are there any signs of occlusion or reperfusion?
Serial ECGs demonstrated dynamic changes diagnostic of ACS (transient STEMI) 4. Finally, Transient STEMI should be taken emergently to the cath lab. Normalization of Diagnostic For STEMI Prehospital ECG with Nitroglycerin Therapy. Learning Points 1. This was diagnosed as a NonSTEMI. Always look at prehospital ECGs 4.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content